Notas metodológicas
← vista completaPublicado el 22 de noviembre de 2024 | http://doi.org/10.5867/medwave.2024.10.2972
Elementos clave para la comprensión y desarrollo de investigaciones cualitativas para profesionales de la salud
Key elements for understanding and developing qualitative research for health professionals
Abstract
Qualitative research plays an essential role in health sciences, aiming to achieve a deep understanding of phenomena, experiences, perceptions, and behaviors in their natural contexts. In this article, we outline essential aspects to consider when conducting qualitative research, starting from formulating the research question to analyzing and reporting the obtained data. We present the main qualitative design methods and sampling techniques, emphasizing the importance of reaching data saturation and the data production methods. This article offers a roadmap for conducting qualitative research in health care, contributing to a more humanized and evidence-based clinical practice.
Main messages
- Qualitative research is an area little explored by health professionals, especially physicians. This type of research provides complementary elements to the findings of quantitative studies due to its ability to explore aspects not captured by the latter and reveal other elements that were not on the researchers' radar, such as people’s perceptions, feelings, and opinions.
- Qualitative designs differ from quantitative designs in that they are flexible in their method, which allows them to be adapted according to the emerging dynamics of the study and the nature of the phenomenon of interest.
- Qualitative data analysis goes beyond the superficial description of the data as it seeks to explore underlying meanings and emerging patterns. To this end, it can use two forms of analysis: content or discourse analysis.
Introduction
Qualitative research is the holistic study of phenomena of individuals or groups in their natural contexts, whose main objective is a deeper understanding of people’s experiences, perceptions, behaviors, and decisions and the meanings attached to them [1]. Their use has been increasing in health, complementing questions of scientific interest that cannot be solved from quantitative approaches [2].
The qualitative study is associated with the constructivist paradigm, which holds that there are multiple interpretations of reality and that the research aims to understand how individuals construct reality within their natural context [3]. This methodology works with a situated reality. This means that it seeks to understand the depth of a phenomenon in a specific context and not the generalization of its results [4]. Like all scientific research, qualitative research is governed by the laws in force in research on human beings.
Intersubjectivity is an essential characteristic of qualitative research. The research process occurs between a subject (researcher) who seeks to solve a scientific health question that happens to other subjects (persons under investigation). Therefore, the subject (researcher) lives the experience of interest, and there is no passive object of research and receiver of an intervention. Consequently, the field to be investigated is influenced by the subjectivity of the researchers and the subjects investigated. Qualitative methodology does not seek objectivity since it assumes that the reality of the subjects is a dialogical construction between them and, therefore, what is observed. Reality is always subjective since it is indebted to the one who observes it [5]. This does not contradict the methodological rigor of qualitative research. As will be mentioned in later paragraphs, there are criteria and techniques to calibrate the subjectivities inherent to the research process with this methodology and to give validity to the results obtained.
This methodology is characterized by using inductive reasoning, given that the researcher begins by exploring a particular context. In addition, a general reality about the facts is given at the end of the research process. On the other hand, although it has a structure, it is characterized by being flexible and open to emerging scenarios, and changes can be made to the method during the study as the facts unfold [1].
The main applications of qualitative research are exploring an unknown topic, studying phenomena that cannot be explained by quantitative research, discovering new points of view, and responding to research problems that lack an objective theoretical hypothesis [6]. In the health area, it has been applied mainly to studying the experiences, perceptions, and attitudes of patients and healthcare providers regarding disease, quality of life, and treatments in general [7]. In addition, it has been widely used to complement quantitative research findings and support the field of public health policy.
This article will address five relevant topics to understand the basis of the qualitative method and to encourage its use in health careers:
-
Context and research question.
-
Methodological designs.
-
Sampling techniques.
-
Information production and data analysis.
-
Quality and reporting of qualitative research.
This article contributes to the methodological series of narrative reviews on general topics in biostatistics and clinical epidemiology, which explore and summarize, in a friendly language, published articles available in major databases and specialized reference texts. The series is oriented to the training of undergraduate and graduate students. It is carried out by the Chair of Evidence-Based Medicine of the School of Medicine of the University of Valparaiso, Chile, in collaboration with the Research Department of the University Institute of the Italian Hospital of Buenos Aires, Argentina, and the UC Evidence Center of the Pontificia Universidad Católica de Chile. This article introduces essential elements for understanding and developing a qualitative study in the health sciences.
Literature search strategy
This review began with identifying key texts in printed versions in the university library. Texts by recognized authors using qualitative methodology written in English and Spanish were used. Subsequently, the information gathered was complemented with scientific articles rescued from databases such as MEDLINE/PubMed, Google Scholar, ScienceDirect, and SpringerLink to delve into methodological designs, sampling, information production strategies, and criteria of methodological rigor.
Context and research question
Qualitative research studies the natural contexts in which individuals or groups develop. That is why, unlike quantitative research, it does not seek to generalize the results but to gain an in-depth understanding of a phenomenon in a given context. Understanding what patients and professionals feel, think, or do in their natural context can help to make clinical practice and evidence-based interventions more effective and humane.
Qualitative research seeks to answer the "what," "how," and "why" a phenomenon occurs in a given context. This requires broad research questions and researchers open to unexpected and changing findings. The production of information and data analysis are iterative and simultaneous processes, so this new information can lead the researcher to ask new questions or refine previous ones to understand the phenomenon better. Qualitative research usually uses "emergent designs", allowing flexibility to the research question if required, as long as it is not radically changed, since this would mean conducting a different study [8].
For the literature search and formulation of the research question, the SPIDER (Sample, Phenomenon of Interest, Design, Evaluation, Research type) tool was developed, adapted from the PICOT tool (Patients, Intervention, Comparison, Outcomes , Results and Time) used in quantitative research [9]. Each of its components is described in Table 1.
Methodological designs
As in quantitative research, the choice of qualitative design will be based first on the nature of the research problem, the research question, and the information to be learned about the phenomenon [8].
Polik and Beck [3] define three major qualitative designs: ethnographic, phenomenological, and grounded theory. However, we will define another one that we believe is relevant to describe since it could be relevant in the context of health research [3].
In order to facilitate the understanding of the designs, examples will be given in each case through the topic of feeding infants under one year of age.
a) Ethnographic designs:
design rooted in anthropology. What characterizes this design is that it seeks to describe people, their customs, and culture in the natural environment where they live [8].
b) Phenomenological designs:
this is a tradition of qualitative study rooted in philosophy and psychology, which focuses on the lived experience of humans. Its focus is describing what all participants have in common about the phenomenon [10].
c) Grounded theory:
with roots in sociology and symbolic interactionism, this design seeks to develop middle-range theories. That is, its purpose is to provide explanations of the study phenomenon based on data collected in the field. This design is preferably used when little or no literature on the problem to be investigated, representing a starting point for understanding some topics. What guides the choice of this design is that the research problem arises due to the interaction between the subjects involved in the problem [10].
d) Biographical or narrative designs:
they focus on life stories as their main object of study. Researchers search the subjects' memory for facts and events of interest to make sense of them in light of the passage of time [11].
Sample configuration
Sampling involves selecting individuals who are relevant to answering the research question. In order to perform this step, a sampling plan, a sample number, and the process for recruiting participants must be established [12].
Sampling in quantitative research is characterized as probabilistic. That is, all population members have an equal chance of being eligible to make up the sample. This is achieved by randomly choosing the observation units, which ensures the absence of bias in this part of the research process. In opposition to these characteristics, qualitative sampling does not follow probabilistic orientations but resorts to its orientations or principles. First, the qualitative sample is smaller than the quantitative sample regarding observation units. These units are chosen strategically to provide relevant information on the study phenomenon and, consequently, can respond to the research objectives [13]. The qualitative sampling plan should then describe how many units of observation it needs to account for the phenomenon and state the strategies it will use to ensure that the findings contribute to understanding the issue of interest. Thus, qualitative sampling establishes an a priori number of participants or groups thought to contribute to understanding the subject of interest. This is known as the sample bootstrap, which can be increased in observation units according to theoretical saturation (explained below).
In qualitative research, there are several ways to configure sampling. The most well-known strategies are described below.
Theoretical or conceptual sampling
This method’s conformation of the sample assumes that the selection of participants is based on the fact that they possess the characteristics or attributes of interest for understanding the phenomenon that motivates the research [14]. What underlies this type of sampling is to ensure, through the selected subjects, the appropriate representation of the theoretical concepts that the research team seeks to understand. An example would be when it is desired to know the perception of the treatment in prenatal check-ups in migrant pregnant women, in irregular migratory situations, and the primary health care of a given commune. Thus, the sampling unit would be migrant pregnant women with an irregular migratory status undergoing prenatal check-ups in primary health care in that commune. Therefore, the pregnant women with these characteristics would be the study sample.
Chain or snowball sampling
The sample is established through crucial informants. That is, a person is identified who has the attributes of interest in the phenomenon to be understood, and he or she is asked about someone he or she knows who has the same qualities or experiences, adding them up to complete a relevant number that accounts for the phenomenon [14]. In other words, one person is asked to refer to another while the information is being produced, and the same individuals report other cases of interest. This type of sampling is especially relevant when working with hidden populations, such as men who have sex with men, people in an irregular migratory situation, and people living with HIV, among others [15].
Convenience sampling
These are samples made up of captive informants or volunteers. It is a less recommended type of sampling since it depends on the accessibility, ease, and speed of access to the subjects, and it is not based on theoretical considerations derived from preliminary knowledge of the phenomenon to be studied [13].
In a qualitative study, the sample size is not fixed prior to responding to the study phenomenon. The vital thing in this type of research, whatever the design and type of sampling selected, is to reach a "theoretical saturation of the data". No new interviews, focus groups, focus groups, participant or non-participant observation, or documentary techniques will lead the researchers to gain further insight into the phenomenon under study [16]. Although some authors suggest several interviews or focus groups according to the epistemological approach [12], it is not established, and reaching information saturation is the key objective.
Information production
As mentioned above, qualitative research seeks to delve into experiences on health-illness-care phenomena, which allows for explaining, describing, or understanding a topic in health. In turn, the methods used to produce qualitative information allow the expression of thoughts, values, and beliefs of those who perceive or experience the phenomenon of interest [8].
Several data production strategies have emerged based on audiovisual or artistic material, physical or cultural artifacts, social networks, or the researcher’s own field notes [8]. Most frequently used in qualitative health research are participant and non-participant observation, structured and semi-structured interviews, focus groups, discussion groups, and documentary techniques (Figure 1) [12].
Qualitative research designs.
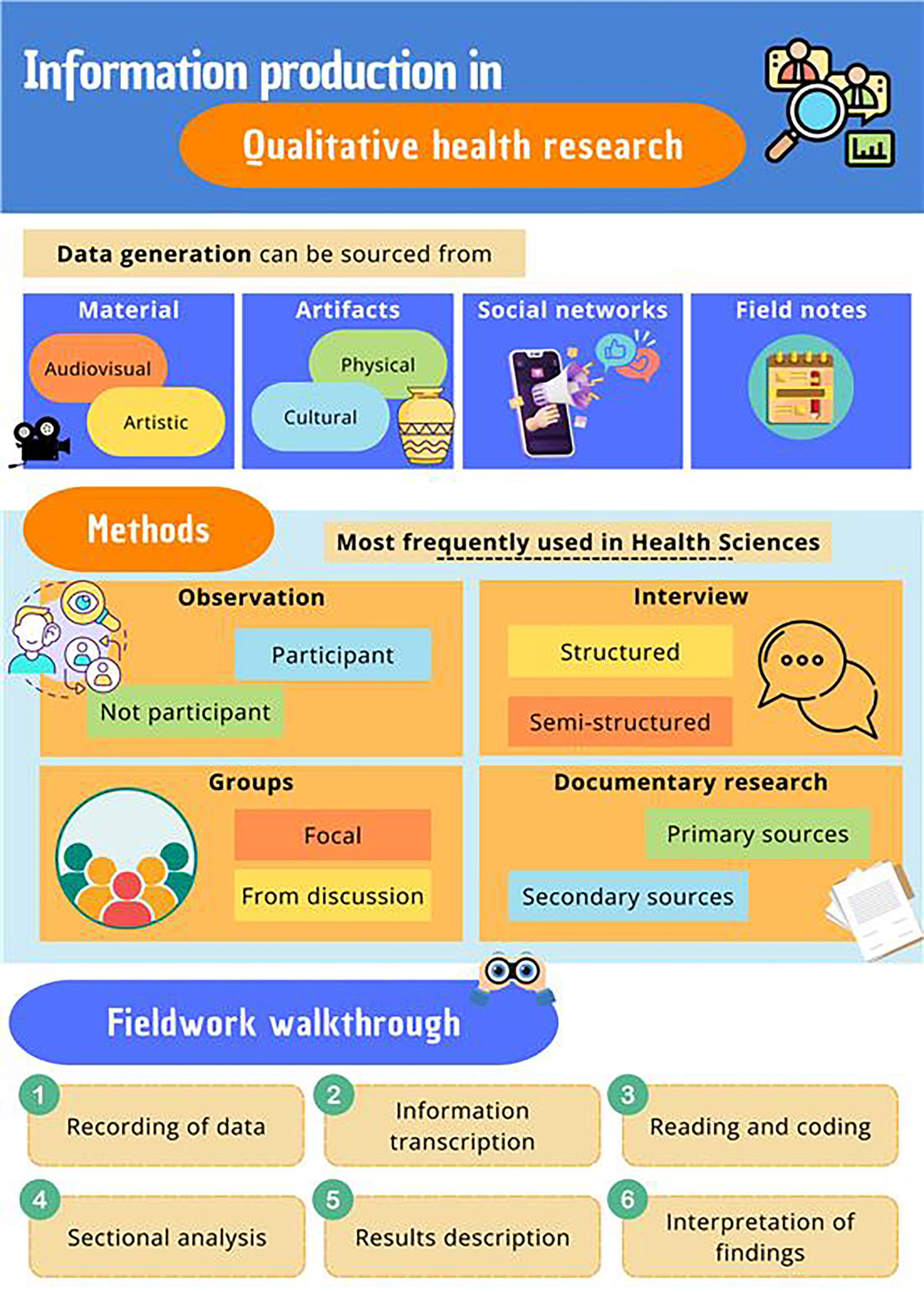
Source: Prepared by the authors of this study.
Table 2 below describes the details of each of the most frequent strategies in qualitative research.
Data analysis
Qualitative information production techniques provide descriptions of the subject matter studied but not explanations. The authors are responsible for posing interpretations of the phenomenon’s eventual relationship or some other association that can be extracted from the data [23].
Often, data analysis in qualitative studies is carried out as soon as the first information begins to be collected or immediately after it has been obtained. Due to the appearance of emerging content, the initial inquiry into these observations may condition how the data continues to be collected or make it necessary to clarify the previous information [23].
Data analysis involves the manual work of researchers based on coding the information obtained to make interpretations and draw conclusions.
In health sciences, two types of qualitative data analysis are frequently used depending on the research objectives: content analysis and discourse analysis.
Content analysis refers to the study of manifest content. The explicit information is expressed directly through the methods and interpretation of its meaning.
Discourse analysis seeks to find the underlying meaning or motivation latently contained in the information collected [17].
The following briefly describes the process for understanding the data produced in fieldwork [17]. It is complemented at the end with Figure 2.
Steps to follow in the fieldwork of qualitative research.
1. Recording or recording of data
This consists of recording the data produced during the fieldwork using audio recording, note-taking, or photographic capture.
2. Listening and writing down the information
In this step, the audio data are transformed into written material through the precise and textual reproduction of the recordings. That is, through verbatim transcription [24]. A faithful copy of the expression of the interviewees should be composed, including interjections, pauses, laughter, noises, and any interaction emitted by the person that is of interest to the analysis.
The files or tapes with the recordings should be stored until the end of the research, each identified with a specific code to maintain confidentiality and certainty of data origin.
3. Reading and organizing the data
It can be considered the first phase of the analysis and is a distinctive feature of the qualitative approach. It is characterized by being descriptive and classificatory. The data obtained are often abundant, so reading the texts exhaustively and repeatedly will be necessary.
In this phase, a kind of dissection of the transcription is carried out. This consists of the selection of short fragments that make sense to the research team because they respond to the objectives of the work or because they represent new information that emerges naturally from the fieldwork.
Each paragraph the researcher selects must be submitted to the coding process, which consists of assigning a label representing the meaning of the identified text segment. These codes, determined by the author’s reflections, may be numerical or visual or use words [25].
4. Analyze the selected fragments
Once the sections or paragraphs of interest in the transcribed texts have been identified, and each has a code, we proceed to group those labels that have some similarity to transform them into categories. The latter must meet five criteria:
-
They must be exhaustive or comprehensive, i.e., they must allow the classification of all the data available.
-
They must be reproducible by a second analyst.
-
Make sense of the study’s objectives and give voice to the informants.
-
Be credible to the subjects of the study.
-
Be different from each other.
After creating the categories, the information related to each will be sought by rereading and classifying the information from each interview and the entire database.
Once this has been completed, we will reduce the data by writing summaries with a description of the information related to each category. This does not yet imply an interpretation of the data.
5. Describing the results
After classifying the data and identifying the information, the next step is describing it. These characterizations are based on the similarities or differences and the contradictions in the contents of the information extracted in the fieldwork.
6. Interpreting the results
Interpretation is the final phase of the analysis. It seeks to establish relationships and provide explanations or hypotheses that give meaning to the findings. This can generate theories that can be confirmed or rejected in a subsequent analysis or another study.
Nowadays, the analysis process can be supported by computer programs. For this purpose, software like ATLAS allows the process to be managed or systematized.ti, NVivo, MAXQDA [26] and Qualtrics [27]. Although they can optimize coding, facilitate the database search process, and connect the phases of the analysis, the data’s interpretation and organization remain the researchers' sole responsibility [17].
Quality and reporting of qualitative research
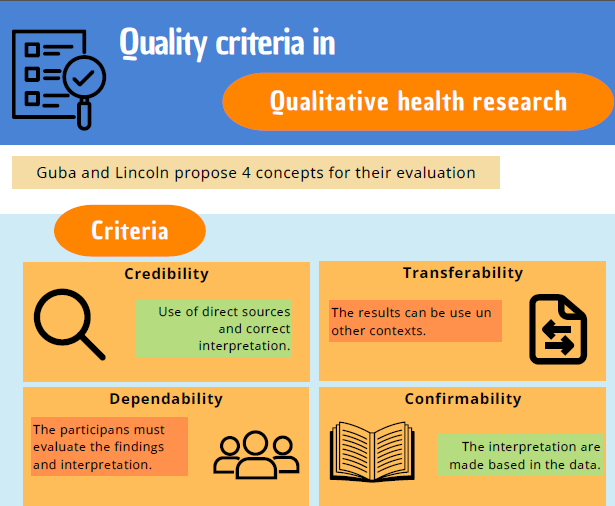
Like all research, qualitative studies have criteria for evaluating their quality. Guba and Lincoln [28] proposed concepts that, although they are not the only ones existing for qualitative research, are widely used in the health sector.
-
Credibility: plausible information is presented from the original data, and their interpretation is correct. It is equivalent to internal validity in quantitative studies. This scope would be achieved by carrying out a series of strategies, such as using the necessary time to get to know the phenomenon and its participant’s persistent observation to identify relevant characteristics and elements.
-
Transferability: the results can be transferred to other contexts. The researcher facilitates the transfer trial with a detailed description.
-
Dependability: stability of the results over time. It involves the participants' evaluation of the findings obtained and the interpretation and recommendations received from the study participants.
-
Confirmability: the results of the research can be confirmed by other researchers. The data and interpretations do not come from the imagination but from the data.
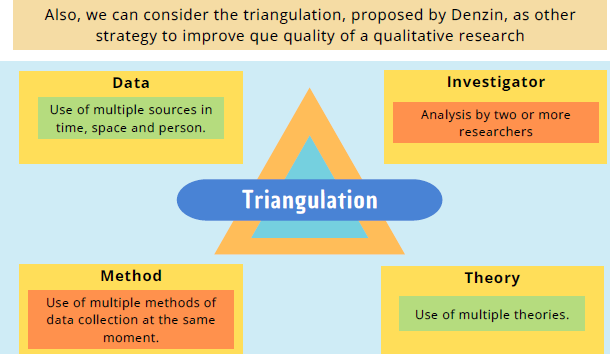
Another component to safeguard the quality of the qualitative study is triangulation. This is a procedure that allows the calibration of the subjectivity that is introduced at the moment of data analysis. In other words, it is a form of validation of the findings [29].
According to Denzin [30], triangulation refers to the search for different perspectives that seek the answer to a phenomenon under study, using different methods or theoretical approaches and that will also be a strategy to deepen the knowledge. Four types are distinguished: methodological, data, researchers and theories. All of them will be described below:
-
Of data: use of multiple sources of data, either in time (different times and dates of publication), space (same phenomenon in other places) and people (search for people of different types and roles).
-
Of researchers: at least two researchers conducting the analysis or interviews, seeking to control or correct biases from individuality.
-
Method: use of different means to collect data simultaneously. Denzin suggests three principles for method triangulation:
-
Consider the nature of the problem to be investigated and the relevance of a particular method.
-
Remember that each method has strengths and weaknesses.
-
The method should be selected based on its theoretical relevance.
Theoretical:
involves approaching the data with multiple hypotheses and theories in mind from various theoretical viewpoints.
Both of these qualitative research quality assurance techniques are summarized in Figure 3.
Quality in qualitative research.
On the other hand, in the member check, the data collected, interpretations and conclusions of the research team are presented to the group from which they were obtained. In addition to the criteria described above, qualitative studies also have their reporting guidelines, which fulfill a similar objective to those used in quantitative studies. Examples of these are the guidelines:
SRQR, Standards for reporting qualitative research. It consists of a list of 21 items that should be present when refueling and writing the results of qualitative research, which are grouped into: title and summary, introduction, methods, results or findings, discussions and others [31].
COREQ [32] Consolidated criteria for reporting qualitative research. This time, a guideline was used to evaluate the methodological quality of the research, with 32 items to be verified, grouped into three domains: research team and reflexivity, study design and analysis, and data reporting. It should be noted that this guideline is designed for studies in which interviews or focus groups are conducted. A version translated into Spanish is available [33].
Conclusions
Qualitative research in the health field is fundamental to obtaining a deep understanding of the phenomena studied, addressing subjectivity, the diversity of contexts, and the complexity of human experiences. Its application requires careful planning, execution, and analysis, as well as following quality and reporting guidelines to ensure the validity and reliability of the results. The use of qualitative methodology in health has experienced significant growth as a sole method and complement to quantitative research.
The qualitative study is associated with the constructivist paradigm, which recognizes the multiplicity of interpretations of reality. It emphasizes the importance of intersubjectivity, where researchers and participants influence the research process. It recognizes that reality is subjective and constructed through the interaction between observers and the observed.
Qualitative research’s methodological flexibility is highlighted, allowing it to adapt to contexts and emergencies during the study. Inductive reasoning is used to explore particular contexts and reach general conclusions about the phenomena studied.
Several methodological designs common to qualitative studies are presented, such as ethnographic, phenomenological, grounded theory, and biographical. In addition, various sampling and information production techniques are described, such as participant observation, interviews, focus groups, discussion or documentary techniques.
The process of qualitative data analysis is detailed, from the production to the interpretation of the data. Methodological rigor strategies are highlighted to guarantee the credibility, transferability, dependability, and confirmability of the results, as well as the importance of triangulation as a validation method.
The SRQR and COREQ reporting guidelines are mentioned, which provide guidelines for writing and presenting qualitative research results, ensuring transparency and methodological quality in communicating findings.
