Notas metodológicas
← vista completaPublicado el 8 de noviembre de 2019 | http://doi.org/10.5867/medwave.2019.10.7712
Enfoque matemático para causalidad prevención-inmigración de brotes de enfermedades de transmisión sexual en Chile utilizando VIH como modelo
Mathematical approach to the prevention-immigration causality of outbreaks of sexually transmitted diseases in Chile using HIV as a model
Abstract
In Chile, in the contingent public debate about the alarming indicators of the prevalence of infectious diseases (such sexually transmitted ones), two factors stand out as determinants: inefficient or scarce preventive campaigns and the poor level of self-care among immigrants. To develop an analytical perspective, a simplified mathematical model is proposed that quantitatively expresses the impact of these factors. Furthermore, we intend to show how these factors working together act within the epidemic of the disease. Despite the simplicity of the proposed argument, a better understanding may address theoretical recommendations for the control and prevention of the disease.
|
Key ideas
|
Introduction
Human migration has historically been acknowledged as an important component in the evolution and interconnection of source/destination countries worldwide[1]. Experts assert the impact of migration dynamics on social patterns in these countries has increased, directly affecting basic aspects of daily life. The sectors most affected by these dynamics include economy, culture, and health[2]. Migration has multiple causes, including economic forces, lack of technology, unstable capital, climate change, armed conflict, and political instability[1]. The objective of this research goes beyond the causes of migration, focusing on its consequences, specifically the health of the host population.
In the Americas, most migration has, historically, been from the South to the more industrialized and technologically advanced economies in the North. However, physical barriers (distance), cultural barriers, and growing administrative barriers have restrained this movement, influencing the destination of new migrants. For many, new alternatives such as intra-regional movement (within Latin America) have emerged as better options. New destinations of choice seem to be societies with some degree of economic stability; geographic proximity; and social, historic, and cultural similarities; for these reasons many migrants have chosen destination countries in the Southern Cone of Latin America[2]. Increasing immigration to Chile reflects this trend. According to Wolff (2017)[3], in the last 15 years, there has been a progressive increase in the percentage of the population living but not born in Chile. In the 2002 national census, for instance, 1.27% of the population in Chile was recorded as migrant. In the 2017 census, this number increased to 4.35% (746 465 immigrants)[4]. According to National Statistics Institute figures, 66.7% of migrants living in the country arrived in Chile during 2010-2017, with the largest populations coming from Colombia, Peru, and Venezuela.
Many research studies have confirmed a close association between global migration and health[1],[5]. However, for various reasons, including the lack of participation of health professionals in global decision-making partnerships, little progress has been made in developing international policies to address this phenomenon[1]. According to a retrospective study on travel and migration in European countries[6], the most commonly reported infectious diseases related to migration are gastrointestinal disorders; systematic febrile illnesses (including malaria and dengue); dermatological diseases (leishmaniasis and leprosy); respiratory diseases (tuberculosis and influenza); Chagas disease; and sexually transmitted diseases (HIV and syphilis). The spread of diseases in the last category are obviously affected by individuals’ awareness of their level of infectiousness or susceptibility, given the option of condom use as a barrier to avoid contagion.
Currently, there has been growing public debate in Chile on the progressive increase in HIV/AIDS infection rates, which have been confirmed by officials from the Ministry of Health Department of Epidemiology[7]. During 2010-2015, for example, 21 856 new cases were confirmed. According to estimates calculated using Spectrum Software (provided by UNAIDS)[7], HIV incidence in Chile is predicted to increase by 5 000 cases per year.
Although migration, as a sociological phenomenon, can affect population health, it does not, by itself, represent a health risk, as stated by Carlos Van der Laat, Regional Health and Migration Officer for the Americas at the International Organization for Migration[8]. However, given that migration can be a factor in disease transmission, our model examined the size of the migrant group that does not follow recommendations aimed to protect people from sexually transmitted diseases.
The epidemiologic impact of migration has not been systematically identified in Chile, as noted by Wolff[3]. However, migration can be a factor in the spread of some diseases, such as cholera, tuberculosis, tropical infectious diseases, and those that are transmitted by vectors, as mentioned in the above-mentioned research. Another group of diseases mentioned in Wolff’s research are sexually transmitted infections (HIV, syphilis, and gonorrhea, among others). This group of diseases attracted our attention in developing this model because the main preventive measure is linked to human behavior.
As mentioned above, current figures for HIV have caused national concern in Chile, and the resulting public / media debate on this issue has increased social speculation regarding causality. In some cases, these speculations have been skewed by political opportunism. Arguments range from slightly technical to completely unscientific, and opinions range from those characterizing increased HIV incidence in Chile as a natural consequence of the high rate of immigration to the country to those that focus on the lack of public policies for the prevention and control of the disease.
After attending a meeting with Minister of Health Emilio Santelices on guidelines for Chile’s new National Plan for HIV, SIDA-Chile president Dr. Carlos Beltrán said, "The HIV problem in Chile is not caused by migrants; it is a problem country-wide." This opinion was supported by Infectologist and Director of the HIV Center of the Clinical Hospital at the University of Chile, Alejandro Afani[9].
Some media and specialist groups assert the main cause of HIV is a lack of effective government prevention measures, including education in the use of condoms. Since the 1990s, the Government of Chile has implemented more than 20 prevention campaigns, but very little effect has been seen within the population. This situation is worth analyzing, given the alarming figures and estimates for HIV incidence. Some important arguments on this subject can be found in two reports: Weaknesses on the Strategy against AIDS[10] and Unforced Failures on HIV Policies[11].
The current study was designed to quantify and compare the effects of prevention policy measures and migration on disease incidence, specifically long-term prevalence, by including a function of susceptible migratory flow and frequency and effectiveness of preventive campaigns. We analyzed a hypothetical sexually transmitted disease scenario where individuals are able to self-regulate (avoid disease transmission) to 100% effectiveness through the responsible use of condoms. The proposed approach is use of a mathematical model (non-statistical approach, with a priori meaning) that assesses the hypotheses using functions[12],[13],[14],[15],[16] and generates a dynamic system using basic impulsive differential equation theory techniques[17],[18].
The novelty of this approach is that it helps supports the development of coherent arguments that should be understandable to a wide variety of audiences without losing scientific accuracy. The main limitation of this study was the use of a highly simplified model that unquestionably omits some variables of the multifactorial phenomenon under study. The strength of the model is the potential for its findings to help put theoretical health recommendations into practice.
Model assumptions
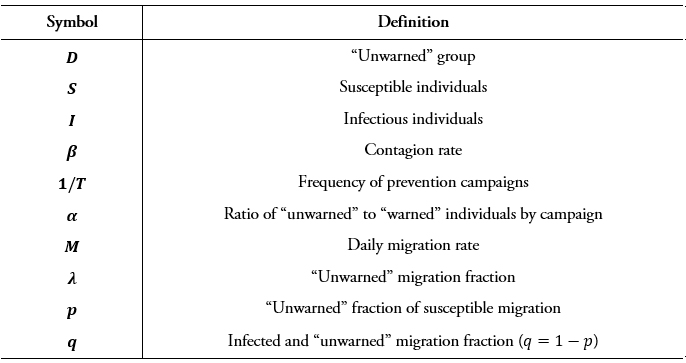
A hypothetical scenario is proposed to simulate contagious infectious disease transmission that requires physical contact between infectious and susceptible individuals. For the purposes of the study, the scale of time from the starting point of the infection to transmission was assumed to be insignificant. In addition, it was assumed that prior to any encounters with the potential for disease transmission, individuals can be classified into two different groups: 1) those that put up behavioral barriers to stop pathogens from being transmitted to another individual, and 2) those who deliberately do not. Individuals who could unknowingly contract the disease as a result of the behavior of the latter group were called the “unwarned” group, and its size at any particular time t lis denoted by D(t) .
The number of encounters that could transmit disease was uniformly distributed within the population, with disease spread occurring from infectious to susceptible individuals belonging to the unwarned groups. The size of these groups on the 10th day are respectively denoted as S(t) and I(t), with β representing the rate of transmission. Daily incidence on the 10th day is expressed as the product of βS(t)I(t), where D(∙)=S(∙)+I(∙), plus the number of external individuals (those from a migrant population).
Our main objective was to depict, within this highly simplified reference framework, two generic mechanisms affecting the spread of the disease: 1) prevention (campaigns promoting change in individual behavior that created a barrier to the spread of pathogens), and 2) the addition of external (migrant) “unwarned” individuals to the population. With respect to these two mechanisms, the following considerations should be taken into account:
a) Prevention: As described above, for the purposes of this study, the population is assumed to fall into one of two groups: 1) those that carry out one single protective behavior (e.g., the use of prophylactics) that is assumed to be completely effective; and 2) those who deliberately do not practice that behavior unless they are encouraged to do so through prevention campaigns (i.e., the study assumed a population can be divided into two groups: people who protect themselves and people who do not). It is also assumed that once a person leaves the “unwarned” group (i.e., becomes informed of the risks) he/she remains in the protected group forever (or at least throughout the study period). Therefore, once a susceptible or infectious individual becomes “protected,” he/she no longer participates in the dynamics of the epidemic. In addition, it is assumed that prevention efforts convert a fraction of the “unwarned” group into members of the “protected” group at each time interval analyzed in the model . Consequently, over time,T, 2T , 3T , …,α(S+I) , of the model population leaves the “unwarned” group.
b) Migration: This model assumes a significant migration flow and (given its short-term time horizon) a constant population (excluding immigration), and variation in these two normally dynamic factors is not considered. Daily migration is denoted by the constant M individuals, and a fraction of the population λ is considered “unwarned.” This latter group is subdivided into “unwarned susceptible” and “unwarned infectious.” Assuming a steady rate of migration, at each 10th-day interval, more pλM individuals are added to the two groups (see Table 1).
 Full size
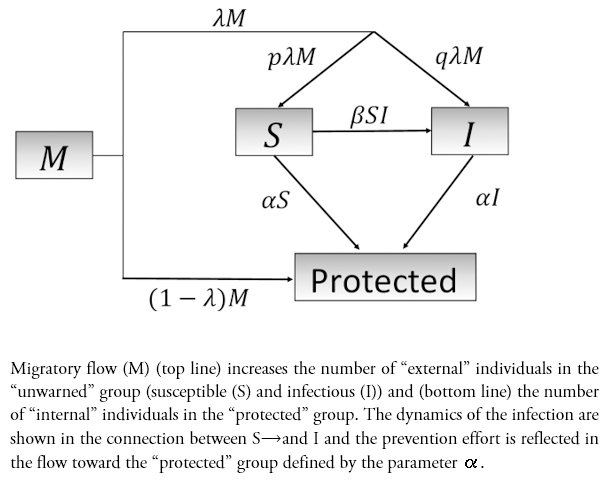
Full size The flow dynamic within this framework and basic modeling of the variation in susceptible and infectious groups (not taking births and deaths into consideration) is shown in Figure 1:
 Full size
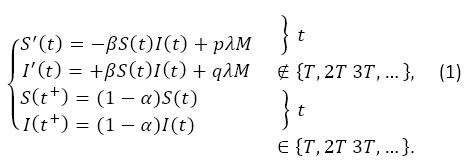
Full size By considering the sum D=S+I, the equations of the system (1), the evolution equation for the “unwarned” group is as follows:

Between two prevention campaigns, the number of “warned” migrants entering the system is denoted by .
Analysis
As shown in equation (2), the total number of “unwarned” individuals in two consecutive time periods, kT and (k+1)T, from two different prevention campaigns, are related by
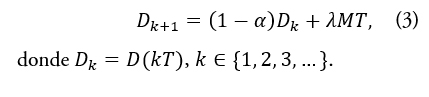
Observation: Considering (3), with an estimated migration (per unit of time) in Mk during the period [kT,(k+1)T], we show that Dk+1 will be, respectively (a) less than, (b) equal to, or (c) greater than Dk , according to:
|
(a) Dkα>λMk T, |
(b) Dk α=λMk T o |
(c) Dk α<λMk T. |
Therefore, based on the number of individuals that the prevention campaigns are able to move to the “warned” group, per unit of time , it is greater than, equal to, or less than the number of “unwarned” individuals who enter the system between the two campaigns λM_k T.
Unique control over the parameters α, λ and T is assumed, and, in order to improve future scenarios, it is necessary to maintain or achieve condition (a), for reduction of the “unwarned” group, which should be reached by implementing a mixture of the following strategies:
Increase α: Attaining condition (a) is not an easy task in a dynamic environment; attempts to reduce risk through behavior change in the “unwarned” group might create opposition to change. In addition, given the short time period that is assumed, the associated costs might rise drastically.
Decrease λ: Migrants face significant challenges upon their arrival in a new country. Therefore, completing an education program before arrival in the destination country might enlarge the “warned” group. Prevention goals might also be achieved by reducing , using entrance barriers, and reducing , by reducing selectivity. However, from a human rights and ethical perspective, these options are not acceptable.
Decrease T: This option requires increasing the frequency (1/T) of prevention interventions or campaigns.
Maintaining a constant migratory rate without intervention on the parameters of (3), by explicit resolution D(∙), is obtained during the time periods nT∈{0,T,2T,3T,…}:
The equation below expresses stabilization (at a large enough size) of the final “unwarned” group, independent of initial size:
This is an expression of the reduction achieved by increasing α and, decreasing λ or T.
Prevalence curve
Using S(t)=D(t)-I(t) in the second equation of (1), the prevalence function satisfied in t∈ ]kT,(k+1)T], the equation is as follows:

with initial condition I(kT+)=(1-α)I(kT), in which D(t) solution of (2).
The analytical information (expressed as equations) for the initial and final values for the infectious group, , is provided in the Appendix.
I∞=lim I(kT)
k→∞ .
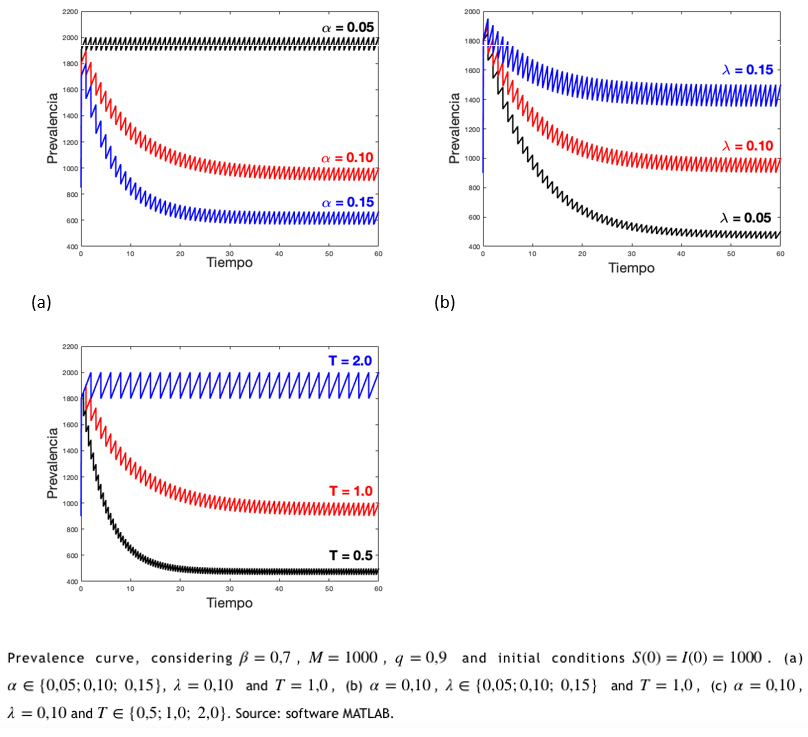
As shown in Figure 2(a), a decreasing prevalence over time is attained by increasing the percentage (5%, 10%, and 15%) of effectiveness for prevention campaigns. The inverse effect is shown in the margins of the final (long-term) variation of prevalence, with a 3:2:1 ratio proportion. Figures 2(b) and 2(c) show a direct effect on prevalence, at each time interval, by increasing the “warned” migrant fraction (5%, 10%, or 15%) or the frequency of the prevention events 1/ (0.5; 1; 2).
Figure 1: Flowchart
 Full size
Full size Discussion
This study proposes a method for developing a stronger analytical perspective in the public debate about HIV in Chile. National concern about the country’s increased HIV incidence has been ignored by the national government thus far due to a lack of coherent, comprehensive, and effective social intervention programming, including prevention campaigns for the high-risk population. Based on the results of the model, the authors recommend joint efforts in designing public policies for control and prevention of the disease, using the parameters described. In practice, the policies should help
- Reduce the fraction of migrants with sexually unprotected (“unwarned”) behaviors (λ);
- Increase the fraction of individuals who move from the “unwarned” to the “warned” condition in term of protection (α); and
- Increase the frequency of public health agency prevention interventions or campaigns against HIV (1/T ).
According to the 61st World Health Assembly, endorsed by WHO[19], as shown in section WHA61.17 (“Health of Migrants”), there is a need for continuous dialog on migration policies among various decision-making sectors. The WHA document also encourages member states to formulate and implement new and better strategies to improve the health and well-being of their populations, in the face of the global migration phenomenon.
Given the current dynamics of migration, a more realistic approach is encouraged[1] for better management of all phases of the process (departure from country of origin, travel period, arrival in destination country) in order to produce more effective intervention policy. In terms of feasibility, interventions implemented during the first phase (preparation for departure) may to lead better results.
In destination countries, several initiatives have proven successful, including one on HIV awareness carried out on the Mexico-United States border with a group of worker migrants that using photo-novellas and radio soap operas[20]. Migrants were informed about HIV testing, effective use of condoms, and recommendations on how to survive the HIV virus. Changes in beliefs and attitudes about the use of condoms and safe behaviors were achieved through the program. Training interventions carried out by “health promoters” from the same community, who delivered condoms and instructions on their use, also showed good results. Similar interventions could be implemented in Chile; if effective, they would benefit the local community as well as the migrant community.
A significant topic linked to the increased number of individuals leaving the “unwarned” group (increase in ) are campaigns designed to identify individuals who are unaware of their health status as carriers of the disease. An HIV-diagnosed person is easier to reeducate and, most likely, change from a susceptible status to abstention on the use of barriers. Between 2010 and 2017, about 3000 to 6000 cases were reported, and in 2018, about 1000 cases. According to the president of SIDA-Chile, Dr. Carlos Beltrán[21], in future it will be possible to reach a large part of the at least 25 000 undiagnosed carriers estimated to be living in Chile.
The effectiveness of an intervention program can make a big difference in terms of social impact[22]. This study proposes a multilevel plan with different options for risk reduction. Campaigns based on abstinence or single partners are now considered inappropriate and inefficient, especially in modern cosmopolitan societies.
The government measure[23] is designed to determine if the search for new cases is effective, since it means increasing or increasing the frequency 1/ , but only when disease carriers actually accept a viral suppression treatment, and an educational intervention, allowing any originally in the “unwarned’ group to move to the “protected” group. However, underestimating the importance of the use of condoms, and focusing on reactive strategies, as has been proposed by the Sida Maule Foundation[24], is not an appropriate response, because there is another option—perhaps more radical—to decrease (see equation (5): increasing . On the other hand, although there is no evidence of higher incidence of HIV among migrant populations, the role of factor , as a fraction of “unwarned” migrants, is one of the direct factors that defines a long-term endemic level.
Notes
Appendix: https://doi.org/10.6084/m9.figshare.10272623
Roles and authorship contributions
FDCL: conceptualization, methodology, formal analysis, research, writing (proofreading and edition), supervision, project management. MGCH: conceptualization, research, writing (proofreading and edition). JPGJ: methodology, research, data management, data presentation, manuscript preparation (development of the original draft), visualization. RIGA: research, data management, data presentation, visualization.
Funding sources
The authors declare that they have received no external funding.
Competing interests
The authors have completed the ICMJE conflict of interest declaration form and declare that they have not received funding for this report; do not have financial relationships with any organization that might have interests in the published articles in the last three years; and do not have any other relationship or activity that could influence this published article. Forms can be requested by contacting the corresponding author or the editorial Chief of this Journal.
Acknowledgment
We would like to thank the Epidemiological Analysis Line of the Doctorate program of Applied Mathematical Modeling at the Universidad Católica del Maule.
