Short communications
← vista completaPublished on September 9, 2022 | http://doi.org/10.5867/medwave.2022.08.002517
Perception on phone medical report to family members of patients admitted by COVID-19 to emergency observation rooms of a tertiary hospital: A cross-sectional study
Percepción sobre informe médico telefónico a familiares de pacientes ingresados por COVID-19 en salas de observación de emergencias de un hospital terciario: estudio transversal
Abstract
Introduction Medical reports of patients admitted to the emergency services has been modified due to the social distancing needed in the COVID-19 epidemic. For this reason, it is essential to know the family members' perceptions about telephone medical reports.
Objective To determine the perception of care by family members of patients hospitalized due to COVID-19 on telephone medical reports in a tertiary hospital's emergency room in Lima, Peru.
Methods A non-experimental cross-sectional study, through a survey of family members of patients with COVID-19 admitted during July and August 2020. The "External user satisfaction survey of the Ministry of Health" adapted to this setting was used due to the absence of similar studies. Information, respect for the user, efficiency, accessibility, suitability, security, and overall satisfaction were considered. The sample size for finite populations was selected from 2 936 family members, obtaining 347 surveys from 641 calls. Relatives were called by phone, and after acceptance, the survey was sent to them via WhatsApp in Google Forms format. Once the survey was received, it was analyzed using descriptive statistical techniques.
Results We made 641 telephone calls with a response rate of 54.1%, obtaining 347 surveys. The mean age was 40.12 years (standard deviation: 11.93 years), with 61.4% of females and 38.0% married. We found that 65.1% received higher education and that Chorrillos was the most prevalent district (10.1%). Moreover, 42.4% of those surveyed were children of hospitalized patients, 17.3% were spouses, and 85% were not health personnel. We found a high level of agreement in overall satisfaction (73.2%) and in most dimensions, including information (88.8%), respect for the user (82.1%), efficiency (70.3%), accessibility (75.8%), suitability (79.0%), and security (87.9%).
Conclusion The telephone medical reports to relatives of patients hospitalized due to COVID-19 in the emergency room found an overall satisfaction of 73.2% . Telephone medical reports are essential alternatives to improve the quality of care during the COVID-19 epidemic.
Main messages
- The COVID-19 epidemic, with its necessary strict biosecurity, directly impacts the doctor-patient-family relationship. Telephonic medical reports are part of the new measures needed to bring the family closer to their hospitalized relatives
- At the time of writing, there are no studies addressing this issue. Thus, it is necessary to know the degree of acceptance of this process.
- A possible weakness of the study is the memory bias of family members when answering the surveys.
Introduction
In December 2019, an outbreak of Coronavirus disease 2019 (COVID-19) ppeared in the city of Wuhan, capital of Hubei province in China, causing a severe acute respiratory syndrome since then called SARS-CoV-2 [1]. On March 11 2020, the World Health Organization (WHO) declared this entity a pandemic. On March 6 2020, the first case of COVID-19 was confirmed in Peru, and by November 29 2020, 958 324 confirmed cases and 35 839 deaths had been reported [2].
Due to high contagiousness, this disease requires strict isolation of patients and medical personnel and restriction of visits by patients' relatives. Moreover, isolation measures restrained the direct contact of the health personnel when submitting medical reports of hospitalized patients diagnosed with COVID-19 to family members. Communication barriers in this context forced physicians to provide medical reports through the Internet and telephone. Other communication modalities, such as WhatsApp, written messaging, voice messages, and video calls, have been reported as valuable tools for healthcare settings [3,4].
The WHO states that e-health consists of "support for the cost-effective and safe use of new information and communication technologies in health promotion and related areas, including health care services, health surveillance and documentation, health education, knowledge and research" [5].
In this context, various forms of telehealth have been implemented, such as live videoconferencing, store-and-forward technology, remote patient monitoring, or texting and emailing. Their purpose was to address developing scenarios that aim for the patient and family care [6,7].
Although the medical act through telehealth has not been clearly defined, the urgency of consultations and daily medical reports to family members of a patient’s state of health in this new context required these actions to be implemented [8].
Despite its relevance, this is the first study addressing this issue in epidemics at the time of writing. Therefore, this work aimed to determine the perception of the quality of care in the telephonic medical report given to relatives of patients admitted for COVID-19 in the emergency room of the Edgardo Rebagliati Martins hospital in Lima, Peru.
Methods
Study design
This is a cross-sectional, descriptive study.
Population
This study included family members of patients admitted to the emergency room due to COVID-19 from July to August 2020 who gave a telephone number and were responsible for receiving medical reports on the evolution of a patient’s health status and others.
Procedure
During the two-month period, 9489 telephone medical reports were recorded, corresponding to 2936 family members. Using the formula for a finite population with 95% confidence, 5% precision, and an estimated parameter proportion of 50%, a sample size of 347 surveys was obtained. Simple random sampling was performed from the list of family members ordered by the date of telephone information until the desired sample size was obtained.
Relatives were included in this study if they completed a survey corresponding to a patient admitted to the emergency department for COVID-19, received a telephone report of the patient’s state of health, and agreed to participate in the study.
Surveys were conducted using Google Forms and were completed by the relatives of patients admitted to the emergency room during July and August 2020.
Family members' information and telephone numbers were obtained from the list of relatives informed by telephone concerning patients admitted to the emergency room. A coordinator, with the corresponding authorization, was in charge of safeguarding the information.
Telephone calls were made to the family members included in the sample to inform them about this study and to ask for voluntary participation. Once their participation was accepted, a Google Forms survey was sent to the participant’s telephone number. Once the survey was answered, it became part of a Google Forms database, which was processed with the SPSS 25 statistical program.
Instrument
We adapted the "External user satisfaction survey of the Ministry of Health" scale for this setting, considering that no study with similar characteristics had been done before [9,10]. The instrument had 14 items using a Likert-type scale with the following response options:
1. I completely disagree.
2. I disagree.
3. I neither agree nor disagree.
4. I agree.
5. I strongly agree.
Subsequently, responses 1 and 2 were classified as 'disagree', 3 as 'indifferent', 4 and 5 as 'agree'. The participants' overall satisfaction was quantified with item 14, classifying those with responses 1 and 2 as 'disagree', 3 as 'indifferent', and 4 and 5 as 'agree'.
On the recommendation of experts at the time of analysis, items were grouped into dimensions. Items 1 and 2 were grouped as 'information' dimension, 3 and 4 as 'respect for the user' dimension, 5, 6, and 7 as 'efficiency' dimension, 8, 9, 10, and 11 as 'accessibility' dimension, 12 as ’suitability' dimension and 13 as ’safety' dimension.
The instrument was submitted to expert judgment, obtaining a content validity coefficient of 0.8822.
Analysis plan
The adequate completion of the data collection form was reviewed. The data were coded and processed using the SPSS 25 statistical package. The data were described using frequency tables, graphs, and summary measures according to the variables analyzed. Frequencies and percentages were applied for qualitative variables, and mean with standard deviation for quantitative variables.
Ethics
Each participant was asked for informed consent, and the objectives and potential benefits of the study were explained to them. The Google Forms survey was sent via WhatsApp if the family member consented. The responses were anonymous. Authorization was obtained from the Specific Research Ethics Committee for COVID-19 (CEIE-COVID19) of the Social Health Insurance (EsSALUD).
Results
A total of 347 surveys were obtained out of 641 calls made, with a response rate of 54.1%. As shown in Table 1, 61.4% of the family members receiving telephone reports were female, and 38.6% were male. The participants ranged from 19 to 73 years, with a mean age of 40.12 years (standard deviation: 11.93 years). Relatives between 30 to 59 years predominated (70%), followed by young adults between 18 to 29 years (24.8%). Thirty-eight percent of the respondents were married, and 37.2% were single. Family members belonged to the districts of Chorrillos (10.1%), Santiago de Surco (6.9%), San Juan de Lurigancho (6.3%), San Martín de Porres (5.8%), and San Juan de Miraflores (5.2%). A total of 65.1% received university or higher education, and 23.1% had a technical degree. Regarding kinship, 42.4% were children of hospitalized patients, and 17.3% were spouses, among which 85% were wives. Moreover, 85% were not health personnel.
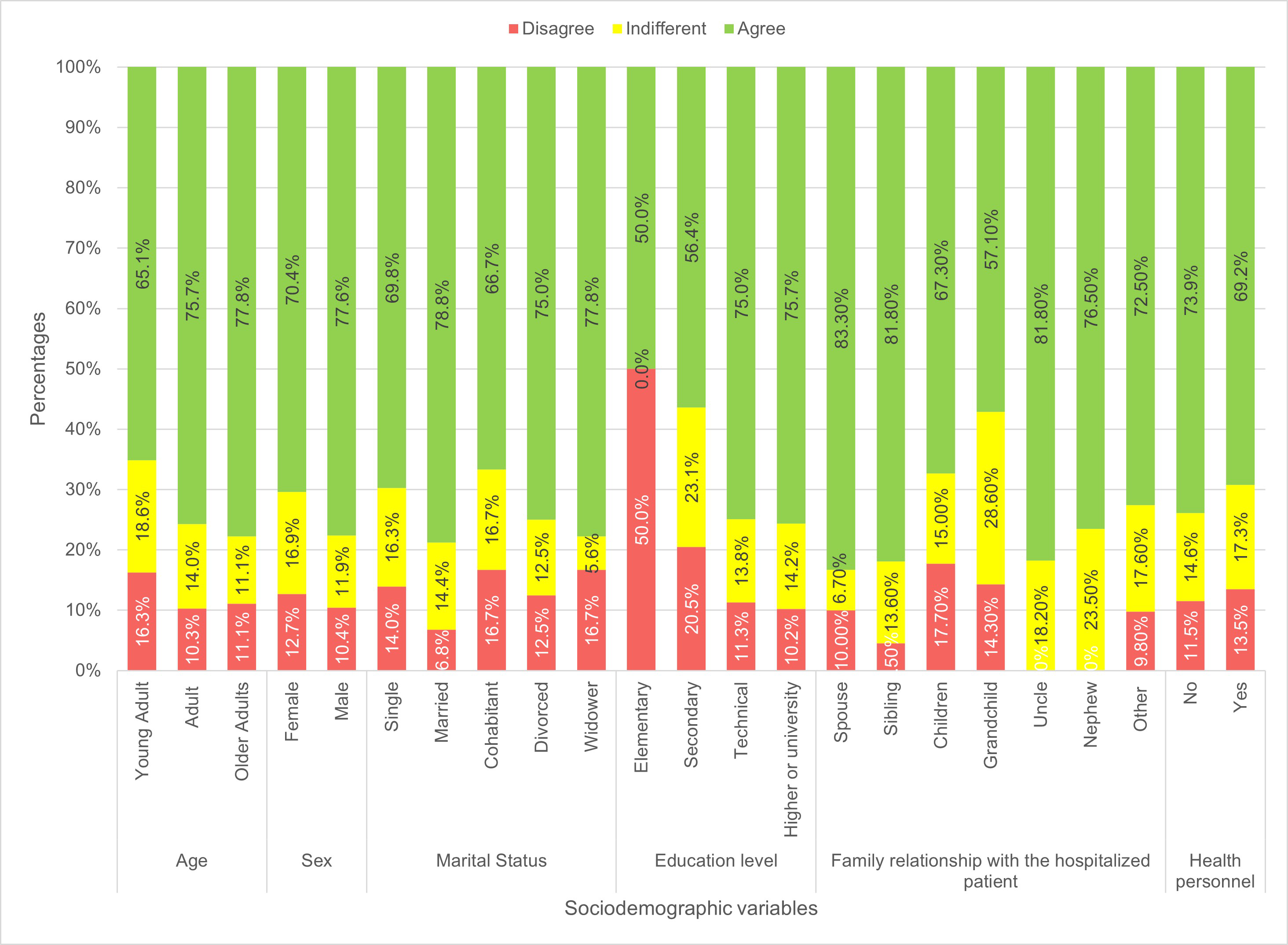
Regarding global satisfaction, Figure 1 shows that older adults (77.8%), males (77.6%), married (78.8%), family members with higher education (75.7%), and spouses (83.3%) presented a higher percentage of the 'agree' response category than other groups.
Overall satisfaction of family members according to their sociodemographic variables.
Source: Prepared by the authors of this study.
 Full size
Full size Moreover, relatives that were not health personnel presented a higher percentage of agreement (73.9%) with survey items than those who were health personnel.
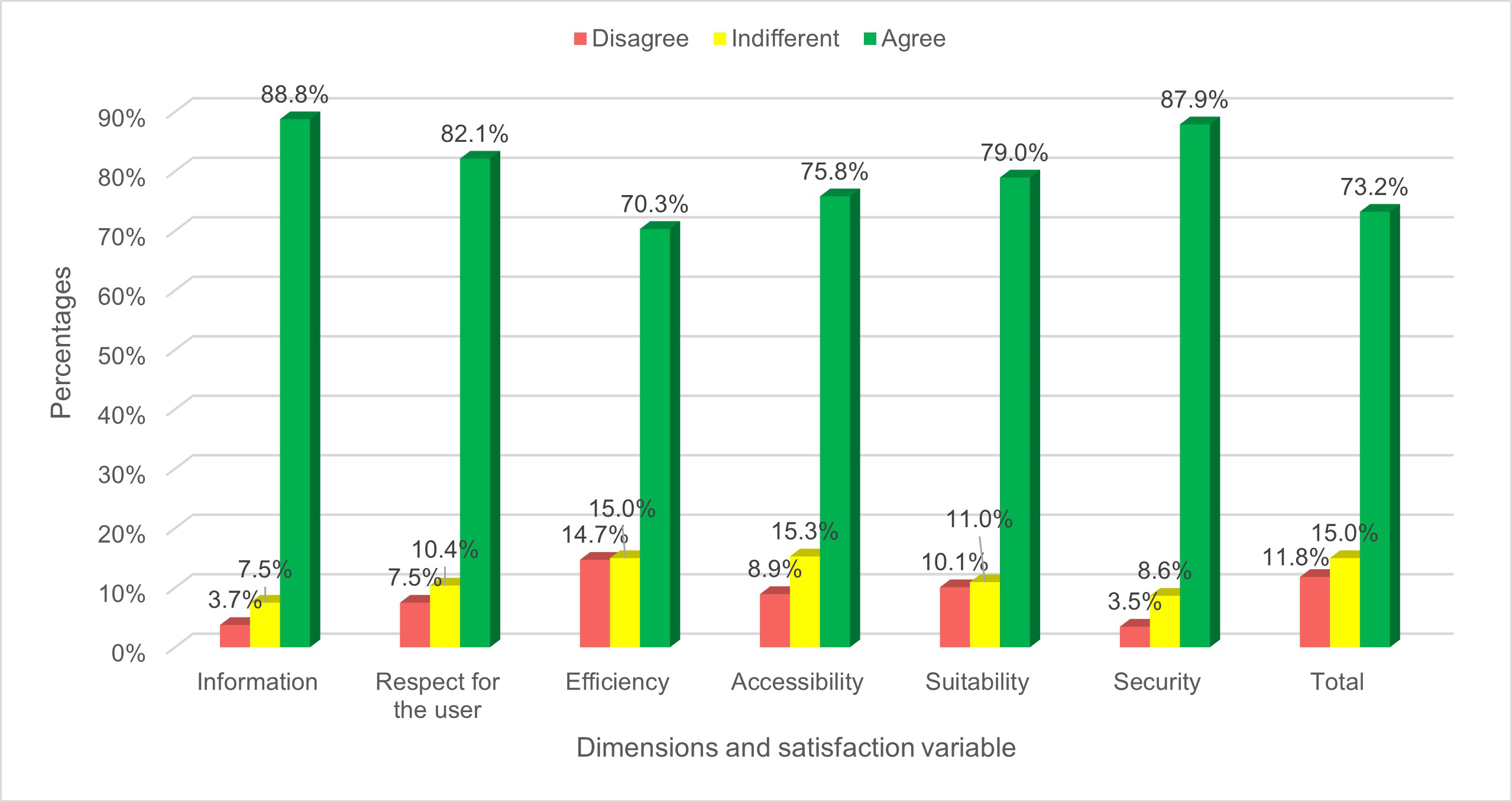
Figure 2 shows a high level of agreement in overall satisfaction (73.2%) and in most dimensions, which included information (88.8%), respect for the user (82.1%), efficiency (70.3%), accessibility (75.8%), suitability (79.0%), and security (87.9%).
Dimensions of family member satisfaction.
Source: Prepared by the authors of this study.
 Full size
Full size Table 2 shows the level of response for each item analyzed, highlighting item 1, which refers to the identification of the caller with 91.6% agreement, followed by item 13, which refers to the privacy of the patient and family member, with 87.9% agreement. Regarding items with the least agreement, item 8 stands out, which refers to the length of the medical report; in this case, 17.9% of the participants reported their disagreement. Moreover, 17.4% disagreed to item 9, which refers to using the telephone as an adequate means of providing this information, and 15.8% disagreed with item 7, related to the usefulness of the information provided to cope with their concern for their family member. However, there was a predominance of agreement in all items.
Table 3 shows the relationship between the sociodemographic variables and the overall satisfaction perceived by the family members. Most family members were adults, female, married, with higher education, and not health personnel. We found that older adults, males, married, with higher education, and not being health personnel, had a higher level of satisfaction with the telephone medical report. The lowest level of satisfaction was found among young female adults with elementary education and among relatives who were health personnel.
Table 4 shows a bivariate analysis between the dimensions and perceived overall satisfaction. We found that more than 80% of relatives agree with the overall satisfaction and the dimensions analyzed.
Discussion
We found that 73.2% of relatives of patients hospitalized due to COVID-19 in the emergency room had overall satisfaction with the telephone information given to them. Likewise – in this first study on the perception of patients' family members – all the dimensions studied obtained levels of agreement above 70%.
Health services management aims to know the quality of care perceived by users to estimate the degree to which the objectives set for user satisfaction are met. Medical information received by the users are indicators of satisfaction and quality of care [11]. In times of epidemics, telehealth has been a fundamental healthcare tool [12,13,14]. Telephone medical reports are part of these actions.
The majority of female relatives surveyed could be related to the preponderance of the male patients admitted to the emergency department for COVID-19. Overall, females were less satisfied with the telephone report, which warrants further studies. The average age of the family member who received the medical report (40.12 years) was related to kinship since children constituted the largest group of family members who received the report (42.4%).
We found a high percentage of relatives with technical and higher level education. This population should have an adequate understanding of medical reports and the survey used in this study, despite the vast majority of respondents not being health personnel. Family members with a higher level of education had higher percentages of agreement with the telephone report. Counterintuitively, family members who were health personnel had a lower percentage of acceptance of the telephone report than those who were not. Their better knowledge of health care and the technical aspects that could have been mentioned in the report may not have determined a better acceptance.
Although the quality of service can be defined as the difference between patients' perceptions and previous expectations [15], we proceeded to describe perceptions in a new and high-impact scenario due to the COVID-19 epidemic. This is linked to the need for information on patient evolution.
In pandemic times, it is essential to inform the family member on the evolution of a disease that may be severe from patient admission. It is worth considering that the medical codes of ethics recognize this right to information [16].
The right to information implies its provision and doing so in the most appropriate manner, which depends on the relative’s characteristics. It is necessary to establish who is the holder of the right to information since there are unique situations regarding the patient’s age and degree of dependence, which, in this epidemic, take on new connotations. Likewise, for a better exercise of the right to information on health-related issues, citizens must have access to good health education [17].
The information dimension obtained 88.8% of agreement concerning who the informant is and its presentation. Considering the effectiveness of the information provided (70.3%), telephone communication in such a challenging environment should be an element to develop and optimize in similar scenarios. The interest in making the family member understand the patient’s health situation and management through the telephone call was perceived as adequate, with 82.1% agreeing on the physicians' respect for the user.
The human dimension evaluates the recognition of a family member as an individual that deserves special attention in a stage of family crisis, where death is around the corner constantly. This requires good communication considering the high psychological impact of these interventions [18].
For this same reason, the central content of medical information should aim to communicate the patient’s evolution and degree of health compromise in the best way possible. In pandemic times, relatives urgently demand information and a correct understanding of the patient’s status; the communication effort of the medical professional should provide complete information and reduce the anxiety and concern of the family members [8,11]. These characteristics – defined as efficacy in information – had 70.3% agreement. These results reveal a good percentage of acceptance.
Empathy with the family members involves delivering, as well as receiving, emotional signals in two-way communication. This is one of the most challenging aspects to develop. It requires time, the duration of which is not yet determined but could be estimated at 10 minutes. The family member should perceive that the data flow is not limited by the time used for it and, consequently, should not feel that time constraints the established relationship [17]. In our study, 62.5% of family members agreed with the time used to deliver the information.
The physician must be prepared to provide adequate information based on technical skills and a psychological attitude that transmits confidence to the family member. Using language understandable to the receiver but without losing precision and empathy, thoughtfulness, truthfulness, and frankness is fundamental [8,11,17]. In this way, the perception of the language used by the physician was 80.7% in agreement.
The communication channel used in this case was the telephone call, and its use obtained 72.9% agreement. This aspect is particularly relevant if key factors are considered. On the one hand, this channel requires an additional effort because the voice is the only tool for transmitting information. Good information and communication must always be kept in mind. On the other hand, the technical aspects of using the telephone must also be considered. Using the telephone without interruptions, in a straightforward manner, with good communication, and without technical problems was perceived by 76.4% in agreement.
All these elements were considered in the accessibility dimension and were perceived as 72.9% in agreement.
Using the evening to call relatives may be adequate since this allows physicians to communicate daily intercurrences, transmit information after working hours, and be more available to respond and listen to the medical report . The appropriateness of the information provided was perceived as 79% in agreement.
Specific considerations surrounding the disease suffered by the patient, as well as the clinical and social background, should be handled by the physician in the light of the right to privacy of information or confidentiality, centered on ethical aspects, and should be perceived as such by the informed family member [19]. These considerations, included in the security dimensions, were rated as 87.9% in agreement.
A possible weakness of the study could be memory bias when answering the survey. However, the characteristics of the diagnosis, confinement conditions, and the worldwide impact of the pathology treated, make such a shocking episode as the COVID-19 disease a vivid memory. The same happens with the report on the evolution of a family member, which may be the only channel of information received from loved ones [14].
Conclusions
The telephone information given to family members of hospitalized patients diagnosed with COVID-19 in the emergency room found an overall satisfaction in 73.2% of cases. This medical information channel may be a good alternative to provide quality care in the COVID-19 epidemic or in situations that prevent contact between medical professionals and family members.
