Estudios originales
← vista completaPublicado el 18 de abril de 2023 | http://doi.org/10.5867/medwave.2023.03.2640
Estudio transversal sobre la calidad de vida y el riesgo psicosocial de trabajadores migrantes
A cross-sectional study on the quality of life and psychosocial risk of migrant workers
Abstract
Introduction Migration figures place Chile as one of the South American countries with the highest rate of migrants. The present study estimated the relationship between sociodemographic characteristics, quality of life, and psychosocial occupational risks in migrant workers from the Maule region.
Methods Cross-sectional study with migrant workers between 18 and 60 years of age residing in the Maule region (n = 145). The applied questionnaires were: a psychosocial risk questionnaire, a health and quality of life questionnaire, and a sociodemographic questionnaire. A bivariate statistical analysis was performed using nonparametric Mann-Whitney U tests, Kruskal Wallis, Spearman correlation, and multiple linear regression models.
Results In Chile, 21% of the migrants maintained the same work activity as in their country of origin. Although the quality of life in physical and mental health is adequate, 52% have low psychological demands at work, 48.9% have low levels of active work and development skills, 57.7% have a high-risk level of compensation and self-esteem, and 65.5% have a high-risk level of double presence at work. Migrants with a higher quality of life in the physical health dimension have a lower risk of maintaining a balance between effort and reward; they worked 44 hours a week and did not work directly at Maule. Migrants with a higher quality of life in the mental health dimension have a lower risk of emotional demands, perceive greater social support in the company, and are less concerned about domestic chores.
Conclusions Migrants with lower quality of life in the physical health dimension presented less compensation at work and recognition, came to work directly in the region, and had jobs with fewer contract hours. Workers with lower quality of life in their mental health exhibited a greater risk of psychological demands at work and perceived low social support in the company; they were concerned about having to respond to domestic and salaried work.
Main messages
- International migration to Chile has increased dramatically in recent years.
- This study contributes to knowledge on the quality of life and psychosocial occupational risk of migrant workers in a region of the south-central macrozone, being a novel initiative that has not been studied before in Chile.
- The study’s limitations are related to the sample size and the non-probabilistic selection.
Introduction
In recent years, internal migratory movements have increased in Latin America and the Caribbean, reaching about 15 million migrants, equivalent to 2.3% of the total population [1,2].
International migration to Chile has increased rapidly in recent years, with an estimated 1 492 522 foreign residents by the end of 2020, representing 8% of the country’s total population [3,4,5]. The above represents almost two times the migrant population registered for 2017, making Chile one of South America’s countries with the highest number of migrants.
The majority of migrants residing in Chile [4] come from Venezuela (30.7%), Peru (16.3%), Haiti (12.5%), Colombia (11.4%), and Bolivia (8.5%). By 2019 in seven regions of the country [6], foreigners from Venezuela exceeded 30%. The three regions with the highest proportion are Biobío (46.7%), Los Lagos (36.5%), and Maule (35.6%), while the three regions with the highest proportion of Haitian migrants are Maule (37.2%), Ñuble (35.1%), and O'Higgins (31.4%).
Evidence shows that immigrant status has relevant implications on the physical and mental health of those affected [7,8]. Studies in the general population have identified risk and protective factors for mental health related to social status, gender, and lifestyle, the interrelationship between physical and mental health, body mass index and diabetes, and genetic and biological factors [9]. However, the mental health of migrants is affected by a wide range of conditions that can exacerbate all of the above, including being away from family and friends and potential vulnerability in the workplace due to over-qualification and low pay. All this leads them to face rejection, social marginalization, and difficulties during the process of assimilation into the dominant culture [10,11]. Exposure to these and other factors can result in various conditions, including maladaptive behaviors and substance abuse, which may affect the migrants' quality of life and environment [12,13]. Further evidence suggests that anxiety and depression have a significant and adverse effect on the quality of life of migrant workers [14,15].
Studies in Latin American migrant populations in agricultural areas of the United States have reported that the presence of depressive symptoms is associated with job insecurity [16] and single workers [17].
Another study conducted in China [18] showed that distressed moods were more prevalent in newly arrived migrant workers, who also had lower wages, recent physical health problems, loneliness, low language proficiency, poor job skills, and long working hours. For migrants in China with more time in the country, depression was associated with low education, recent physical health problems, and low job stability.
Other studies show that variables such as age, health problems, poor coping skills, psychosocial stressors in the workplace, poor working conditions, low wages, workplace harassment, limited access to medical care, length of a residence visa, living conditions, and poor social support networks are associated with depressive and anxiety symptoms in migrant workers [19].
In addition to the above, other factors associated with psychiatric morbidity risk in migrant workers are traumatic events before migration, unplanned or illegal forced migration, low levels of acculturation, family separation, and perceived discrimination. Language proficiency, family reunification, and perceived social support reduce the likelihood of presenting a mental health disorder [20].
In Chile, a study developed in the north [21] on quality of life and well-being revealed that the best-evaluated domain was physical health, possibly since most participants were young adult migrants. However, the worst evaluated domain was the environmental domain due to the difficulty of accessing public health care. It was also found that those migrants who maintained close friendships with people from the host country reported better quality of life than those who did not have substantial relationships with Chilean people.
Another study [22] showed that 22% of Colombian migrants and 13.8% of Peruvian migrants presented anxious and depressive symptoms. At the same time, in the Peruvian and Colombian populations residing in Arica, Antofagasta, and Santiago, a high presence of symptoms associated with difficulties in social interaction and social role adjustment was observed.
A study that evaluated the mental health status of migrants from northern Chile and the relationship with their acculturation strategies and nationality [23] showed that symptoms of depression and anxiety were associated with a high level of acculturation stress experienced by the participants (stress derived from the fact of migrating), distance from the country of origin (homesickness), discrimination and the use of an acculturation strategy (that is, the extent to which the person adopts Chilean customs or maintains those of his or her country of origin) linked to assimilation and marginalization.
No research in Chile addresses the occupational psychosocial risks faced by migrant workers, and national studies on this subject are scarce. A study based on the responses of Chilean healthcare workers in three healthcare centers [24] found high occupational psychosocial risk in all centers, identifying double presence (increased workload due to the demands of the domestic environment) as the most prevalent psychosocial risk factor. In addition, the study found a higher prevalence of risk for workers in emotional and psychological demands, hidden emotions, and sensory demands at work.
Another study, based on mining workers in Chile [25], revealed that most of the risks correspond to the dimensions of active work, development possibilities, social support from the employer, leadership quality of supervisors, remuneration, and double presence, all of which indicate that at higher perceived psychosocial risk at work, the lower the job satisfaction of workers.
On the other hand, specialists affirm that even though the migratory phenomenon in Chile has been a consolidated reality in recent years, there is still little research on the subject, especially in the central-southern part of the country [26]. For this reason, assessing whether occupational psychosocial risks affect the physical and mental quality of life of a heterogeneous group of migrant workers [27] will allow a better description of this population group’s current labor situation. In addition, it will provide useful inputs for future interventions in the field of occupational health, which could apply to migrant populations in intermediate regional cities with characteristics similar to those of the Maule region, where the urban meets the rural in an integrated manner [28].
Our study aimed to estimate the relationship between sociodemographic characteristics, quality of life, and occupational psychosocial risks in migrant workers in the Maule region.
Methods
Participants
A cross-sectional design study was conducted with non-probabilistic sampling. The total migrant population in the Maule region reported in the 2017 CENSUS [29] corresponded to 10 780 foreign residents, where 85% were considered active population (n = 9163). The sample size estimate was calculated for correlations based on a study that evaluated the overall perceived quality of life in Colombian migrants in Chile and its relationship with the variables of income level, cohabitants, and age [10]. We considered a level α = 0.05 (significance level), a level β = 0.20 (1 minus the power, which is = 0.80), and the correlation coefficient r = 0.28 was calculated considering the r2 = 0.078 reported by the model, reaching a minimum sample size of 98 migrants. The final sample comprised 145 working migrants of 12 different nationalities between 18 and 60 years of age, with work contracts and residency in the four provinces of the Maule region: Talca, Curicó, Linares, and Cauquenes. The distribution of the surveyed migrants was 86 individuals in Talca, 40 in Curicó, 11 in Linares, and eight in Cauquenes, corresponding to 59%, 28%, 8%, and 6%, respectively, of the total sample. Some 55% had higher education studies.
The study was developed from October 2019 to January 2020. The study participants were convened with the support of organizations linked to the care of migrants in the region, applying the interventions in the physical spaces these organizations could provide.
The study’s objective was explained to each participant, who later signed an informed consent form. The study was reviewed and approved by the Scientific Ethics Committee of the Catholic University of Maule (Registration No. 222/2019).
Data collection instruments
The questionnaire has 20 closed-ended psychosocial risk questions comprising scores from zero to four, representing levels rated as always[30], most of the time, sometimes, only a few times, and never. The instrument is validated in the Chilean population and presents a Cronbach’s α = 0.70 to 0.80, indicating good internal consistency [31]. It consists of five dimensions and 19 subdimensions that make up and define each dimension, detailed below:
(D1) Psychological demands at work: includes qualitative items (emotional, creative, and sensory demands) and quantitative items (quantity, pace of work, and distribution of work). It is made up of five sub-dimensions:
-
Quantitative psychosocial demands.
-
Cognitive psychological demands.
-
Emotional psychological demands.
-
Psychological demands for hiding emotions.
-
Sensory psychological demands.
Each subdimension is represented by one question (five in total). The maximum score for this dimension is 20. The low-risk level is represented by scores from zero to eight, the medium-risk level corresponds to scores between 9 and 11 points, and the high-risk level is for scores between 12 and 20 points.
(D2) Active work and skills development: refers to the worker’s autonomy in terms of schedules, working pace, applied methodology, variety, initiatives, and quality of work. It has, in turn, five sub-dimensions:
-
Influence.
-
Possibilities of development at work.
-
Control over work time.
-
Sense of work.
-
Integration in the company.
Each subdimension of this dimension is represented by one question (five in total). The maximum score for this dimension is 20. The low-risk level is between zero and five points, the medium-risk level is between six and eight points, and the high-risk level is between 9 and 20 points.
(D3) Social support in the company and quality of leadership: constitutes the capacity for social support provided by the work environment and individual supervision conditions. The sub-dimensions are as follows:
-
Role clarity.
-
Role conflict
-
Quality of leadership.
-
Quality of relationship with superiors.
-
Quality of the relationship with co-workers.
Each subdimension is represented by one question (five in total). The maximum score for this dimension is 20. The low-risk level is between zero and three points, the medium-risk level is between four and six points, and the high-risk level is between 7 and 20 points.
(D4) Compensation and self-esteem: refers to the imbalance between reward and effort, maintaining control of status or anything related to their job stability, and the existing control between undesired changes in their work. The sub-dimensions are:
-
Esteem.
-
Insecurity regarding the general conditions of the contract.
-
Insecurity regarding the specific characteristics of the job.
Each subdimension is represented by one question (three in total). The maximum score for this dimension is 12. The low-risk level is from zero to two points, the medium-risk level is from three to five, and the high-risk level is from 6 to 12.
(D5) Double presence: includes all concerns associated with household chores, children, relatives, and work-related duties. The associated subdimension is: concern about household chores manifested in two questions. The maximum score for this dimension is eight. The low-risk level is between zero and one point, the medium-risk level between two and three points, and the high-risk level between four and eight points.
Calculation and interpretation of the scores are made directly with the sum of the points obtained for each major dimension. The proportion of workers according to risk level (low, medium, and high) can be calculated. The higher the score, the higher the psychosocial risk.
B) Health-related Quality of Life Questionnaire (SF-12)
The SF-12 questionnaire version one [32,33] has 12 items and provides a health status profile applicable for general and clinical populations with a minimum age of 14. It has an acceptable internal consistency with Cronbach’s α = 0.89 [34]. The instrument assesses individuals' physical and mental health-related quality of life and functional status. The SF-12 is a short version of the SF-36 questionnaire. It includes two dimensions [35]: physical health (PCS) and mental health (MCS), along with eight health concepts (physical function, social function, physical role, emotional role, mental health, vitality, bodily pain, and general health). Responses are rated on dichotomous, Likert-scale measures ranging from lowest to highest intensity or frequency of health status. Finally, response scores are summed overall and for both dimensions. The raw scores of the 12 questions are also standardized by placing them from 0 to 100 points. The lower the score, the lower the quality of life associated with physical or mental health.
C) Sociodemographic questionnaire
Designed by the research team to inquire about each individual’s attributes: gender, age, nationality, residence (six questions); educational level (one question); work and employment conditions (five questions). In addition, four questions were asked related to work experience in their own countries and other countries before arriving in Chile.
Data analysis
An initial exploratory analysis of the data was carried out, which included a review of missing data, outliers, duplication, distribution of the variables, and evaluation of the graphic representations. The categorical variables were defined as gender (male and female), province (Talca, Curicó, Linares and Cauquenes); nationality (according to country of origin), marital status (single, divorced, widowed and married), age range (18 to 24 years, 25 to 34 years, 35 to 44 years, 45 to 54 years and 55 to 64 years), level of education (incomplete or complete primary school, incomplete or complete secondary school, incomplete or complete technical, incomplete or complete university and incomplete or complete postgraduate degree), type of contract (fixed term, indefinite term, indefinite contract, work contract and part-time or part-time), working hours per week (29 hours or less, 30 to 43 hours and 44 hours), monthly income in Chilean pesos (from 100 to 300 thousand pesos, from 301 to 600 thousand pesos and more than 601 thousand pesos) and initial region of arrival in Chile (Maule, Santiago and another region); with a nominal scale or with an ordinal scale, according to the characteristics of each one. The variables age, quality of life (physical health dimension and mental health dimension), psychosocial risk at work (psychological demands at work dimension, active work, and skills development dimension, social support in the company and quality of leadership dimension, compensation and self-esteem dimension and double presence dimension) were considered for this analysis as continuous quantitative variables. They were analyzed with measures of central tendency (mean, median) and dispersion (standard deviation and interquartile ranges). The five dimensions of the ISTAS-21 were also analyzed as categorical according to their risk levels (high, medium, and low) in order to describe the risk proportions for each one. Subsequently, the Shapiro-Wilk test was applied in order to evaluate the normal distribution of the variables that measured quality of life (physical and mental health) and psychosocial risk in migrants' work. Since the variables were not normally distributed (P < 0.001), a bivariate analysis was applied with nonparametric comparison tests, including Mann-Whitney’s U test and Kruskal Wallis and Spearman’s correlation analysis. The accepted significance level was less than 0.05.
Finally, two multiple linear regression models were applied to explain the relationships between the variables with the results of the quality of life dimensions related to physical and mental health as dependent variables and with the psychosocial risk at work and sociodemographic variables as independent variables. The model coefficients were estimated with a 95% confidence interval. For the selection of the independent variables in the model, theoretical criteria were considered (according to the dimensions underlying the instruments of quality of life and psychosocial risk at work), epidemiological (according to what is indicated in the literature on variables associated with quality of life and psychosocial risk at work, described in the introduction) and statistical (we included those variables that in the bivariate analysis presented a P < 0.05), using the backward elimination method (which consists of introducing all the variables in the model and then excluding one by one the least influential variable with the largest P value), leaving in the final models the variables with a P < 0.10 and interpreting as statistically significant the variables with a P < 0.05. Qualitative independent variables with more than two categories were transformed into dummy variables or dummies, where they are numbered "1" if the observation had the observed characteristic and "0" if it did not (this would be the reference value of the variable). The analysis of dependent variables corresponding to the quality of life questionnaire results was performed separately (one with the physical health dimension and the other with the mental health dimension). The analyses were conducted with the statistical program Stata 13.0.
Results
The participants' general characteristics are shown in Table 1. The average age was 35 (minimum 19 years and maximum 58 years).
It is observed that 66% were males, and 62% were single, widowed, or separated. In addition, 66.2% of the workers had a full working day of 44 hours per week, 57.2% earned more than 301 000 Chilean pesos, and 56.5% had an indefinite contract.
Only 21% of migrant workers maintained the same work activity as in their country of origin. Regarding current employment distribution, the largest percentage is engaged in the agriculture, livestock, forestry, or fishing sectors (19%). Fifteen percent work in the manufacturing industry. Eleven percent work in wholesale and retail trade, repair of motor vehicles and motorcycles, and another 11% in accommodation and food service activities. Construction activities accounted for 9%, 6% worked in administrative and support services, 8% in other service activities, and 6% in professional activities related to scientific and technological work in universities or research centers. In the transportation field, 3% work in transportation, 3% also work as employers in household activities, and undifferentiated activities of households as producers of goods and services for their use. Another 2% work in teaching activities, another 2% in information and communication activities, and another 2% in human healthcare and social assistance activities. The remaining 3% are engaged in activities associated with the supply of electricity, gas, steam, and air conditioning, financial and insurance activities, artistic, entertainment, and recreational activities, and other undeclared activities.
Regarding work performed in the country of origin before arriving in Chile, 11% of the migrants worked in the manufacturing industry, 10% in the education sector, 6% worked in the supply of electricity, gas, steam, and air conditioning, and another 6% worked as professionals in healthcare centers and performed social assistance activities. In addition, 8% were engaged in administrative and support service activities, while 9% worked in construction and another 9% in wholesale or retail trade and motor vehicle repair. Eight percent worked in professional scientific-technological activities in universities or research centers. Five percent were engaged in accommodation and food service activities, and another 5% in agriculture, livestock, forestry, and fishing services. Eight percent were engaged in undeclared activities. Three percent were engaged in transportation and another 3% in other service activities. A further 3% worked in financial and insurance activities. 1% worked in artistic and entertainment activities and another 1% in household activities as employers, undifferentiated activities of households as producers of goods and services for their use. Finally, 4% worked in more than one of the abovementioned activities in their country of origin.
According to the ISTAS-21 level of psychosocial risks at work (Table 2), it was observed that a significant proportion had low psychological demands at work (52.4%), low levels of active work and development skills (49%), low levels of social support in the company and quality of leadership (37.2%), high-risk level in compensation and self-esteem (51.7%), and a high-risk level of double presence at work (65.5%).
The results of each subdimension revealed a significant risk in psychological and sensory demands (82.7%) and a high level of risk caused by double presence due to concerns over domestic chores in the work environment (50.3%).
The bivariate analysis (tables 3 and 4) revealed that in the psychological demands at work dimension (D1), there were significant differences among the initial region of arrival in Chile (P = 0.024). In the social support in the company and quality of leadership dimension (D3), there were significant differences between groups in the variables: level of education (P = 0.038) and initial region of arrival in Chile (P = .001).
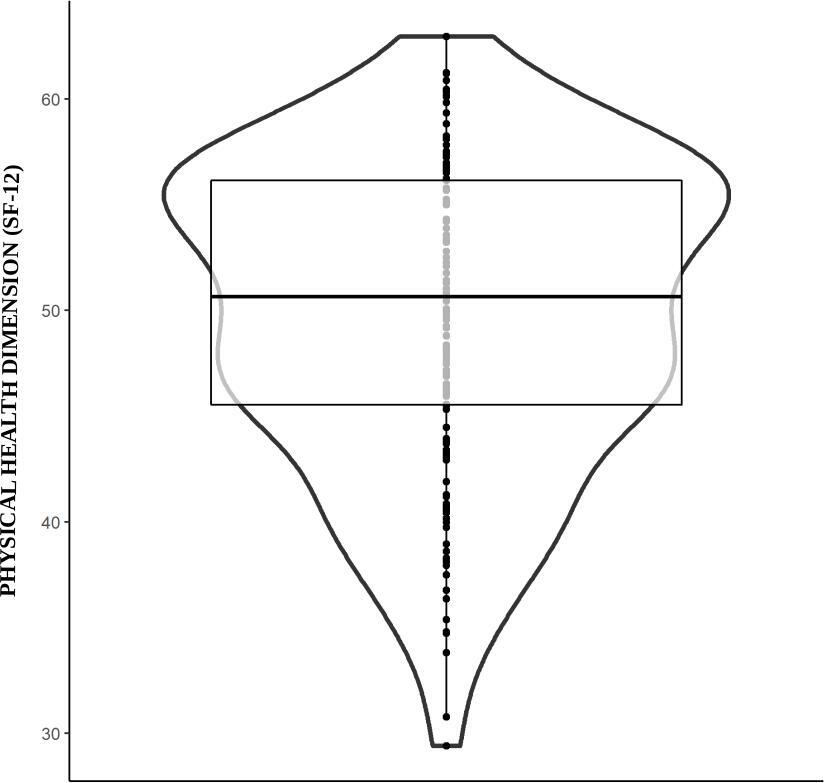
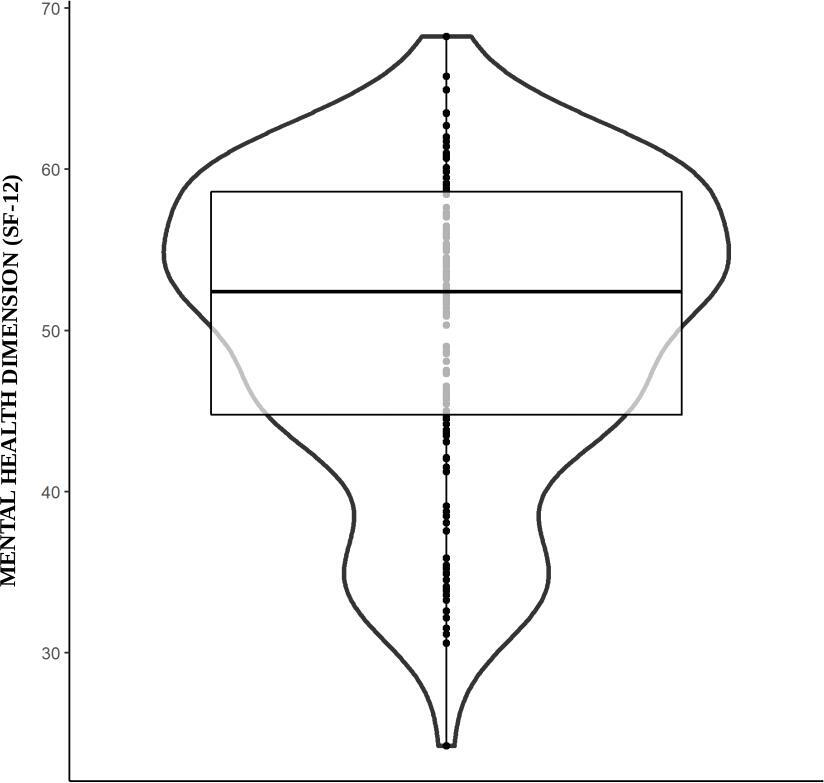
Figure 1a shows in the physical health dimension a median of 50.6 with interquartile ranges of Q1 (25%) = 45.5 and Q3 (75%) = 56.1. The mean was 49.7 (SD = 7.5), with a minimum value of 29.4 and a maximum of 62.0. Figure 1b presents a median of 52.3 in the mental health dimension with interquartile ranges of Q1 (25%) = 44.7 and Q3 (75%) = 58.6. The mean was 50.4 (SD = 9.1), with a minimum value of 24.2 and a maximum of 68.2. In summary, most of the migrants in the study have scores within the expected range in terms of quality of life associated with the physical and mental health dimensions.
Regarding the physical health dimension (Table 5), a statistically significant difference was observed in the quality of life measured with the SF-12 between the marital status of migrants (P = 0.010), type of work contract (P = 0.046), hours of work per week (P = 0.043) and initial region of arrival in Chile (P = 0.002). In the mental health dimension, there were no significant differences between the sociodemographic variables of the migrant workers.
When Spearman’s correlation analyses were performed (Table 6), moderate and negative associations (p less than 0.05) were observed between the mental health dimensions and the psychological demands of the job (rs = -0.416), and the social support at work dimension and the supervisor’s leadership quality (rs = -0.433). A weak negative association was observed between the compensation, self-esteem, mental health dimensions (rs = -0.275), and double presence (rs = -0.274).
On the other hand, regarding the perceived quality of life in the physical health dimension and the psychosocial occupational risks reported by the migrants, a weak and negative association was found between the social support at work dimension and the quality of leadership (rs = -0.175); a weak and negative association was also found for the compensations and self-esteem dimension (rs = -0.169).
Table 7 shows the final multiple linear regression models with the best goodness of fit for the physical health and mental health dimensions, respectively. The models finally included the variables with a P value < 0.10 and with the best R2 (goodness of fit) representing the percentage of variation in the dependent variable explained by the independent variables selected in the model, i.e., the model with the highest R2 was chosen.
In the first model (Table 7), the physical health dimension is negatively associated with a higher risk in the compensation and self-esteem dimension, with the initial region of arrival in Maule, and it is positively associated with working 44 hours per week in contrast to working 29 hours or less. Monthly income and marital status are variables that influence the proportion of the total variance of the dependent variable explained by the model (18%) but do not present a significant association (P < 0.05) with the quality of life associated with physical health. In summary, those who have a higher quality of life associated with physical health have a lower risk of maintaining the balance between effort and reward or maintaining job stability and control between undesired changes in their work, have a job with 44 hours per week (i.e., a full-time job) and did not come to work directly in the Maule region.
In the second model (Table 7), the mental health dimension is negatively associated with a higher risk in the psychological demands at work dimension, higher risk in the social support in the company and quality of leadership dimension, and higher risk of double presence. The total variance of the dependent variable explained by the model is 34%. In summary, migrant workers who present a better quality of life in the mental health dimension have a lower risk in the emotional, creative, and sensory demands and the quantity, rhythm, and distribution of work; they perceive better social support in the company and good relationship with superiors and co-workers; and less concern for domestic chores while at work.
Discussion
Results show that migrant workers in the present study had an adequate quality of life. When compared with a previous work that evaluated the quality of life using the same instrument in Chilean, Peruvian, and Colombian populations, it was observed that they presented lower mean scores in the physical and mental health dimension than migrants working in the Maule region [36]. However, the minimum and maximum ranges showed significant variability in the data (this should be considered) by including a group of migrants with risk in their quality of life in both physical and mental health, considering that 10% of the migrant population presented a high level of risk in both the physical and mental health dimensions.
On the other hand, migrants who presented lower quality of life in the physical health dimension experienced lower rewards or compensations at work, low recognition from their bosses for their efforts, came directly to work in the Maule region from their countries of origin and did not have a full working day. This can be linked to previous studies where limited support networks, isolation, job insecurity, and poor recognition are some of the conditions that affect the well-being and mental health of migrants [7,21]. Workers with fewer working hours and adapting to regional characteristics have less income than full-time workers. They must make greater efforts through other non-formal means to obtain enough resources to subsist [18,19] and have greater expectations of recognition for their efforts. In addition, they perceive fewer possibilities for promotion, the received rewards are unrelated to their capabilities, or they are overqualified for the task [37].
On the other hand, workers with lower quality of life in their mental health perceive that the amount of work exceeds the time they have available to perform their multiple tasks. They feel a high cognitive, sensory load, and emotional demands at work and hide their emotions for professional reasons. At the same time, they present little clarity and conflict in their work role, low support from the boss, and difficulties in their relationship with superiors and co-workers. These data are novel and have not been reported in previous research on psychosocial risk at migrant work. Still, it is very similar to the results found in Chilean mine workers who also perceived little social support from their employers [25]. At the same time, it could be related to inadequate working conditions, poor coping skills, and psychosocial stressors in the workplace [19,20].
Perception of double presence is also observed, which causes uneasiness when feeling that home requirements may impair work performance. Although there are studies that suggest that people with temporary jobs perceive less social support and difficulties in their mental health [37,38], the results found could be explained by the stress of maintaining a stable job in a work environment with low recognition and little control on the workers' behalf, and with the feeling that this job was not what was expected [39].
Similar to research conducted with the Chilean population [24,25], it was found that the psychosocial risks of migrants related to double presence appear to be the dimension with the highest level of risk. An evident concern should be addressed in those who simultaneously perform domestic and work activities.
Psychosocial occupational risks, together with migrant status, are factors that increase adaptation difficulties and consequently affect the mental and physical health of workers [40]. Situations of discrimination and the condition of acculturation [23] could cause alterations in mental health that the literature reports, especially in cases of migrants who do not master the country’s language and are alone [20].
In this study, a novel finding is that migrants who arrived for the first time in a different area of the country and not in the Maule Region perceived less psychosocial risk at work. In this sense, adaptation to the conditions of the new country takes place better in cities outside the region, which allows migrants to successfully settle in and better internalize cultural adaptation, overcoming aspects associated with work stress [21].
Exposure to a new culture can provoke different psychological responses in which anxiety, confusion, and culture shock affect the mental health of individuals [41]. This complex process requires professional support and accompaniment to overcome it. The Maule Region comprises at least four relevant intermediate cities with high agricultural and livestock activities that, although not well known internationally, have an ethnic diversity between rural and urban areas [26], which add richness to the analysis of the quality of life and psychosocial occupational risk of migrant workers in the region [42]. This region also presents a constant internal migration between rural and urban areas that combine homogeneous and historical folkloric traditions, mainly in south-central Chile [42].
Therefore, adaptation begins with understanding the verbal and nonverbal codes of the diverse environments where people interact and live with their original cultural traditions at home and work. The experience of cultural assimilation, not feeling rejected in either environment (one’s own and the new culture), contributes to psychological adaptation, overcoming migratory grief, and effective sociocultural inclusion [13,23,43].
This study shows the need to develop induction training for migrants who have recently arrived in a work area, to strengthen the capacity of institutional and government information offices at health and other basic services fundamental to ensure the correct advice required by migrants. On the other hand, training employers in labor inclusion and migration issues is essential to generate healthy and intercultural work environments. Although some studies reveal successful experiences implemented in countries with high migrant populations [44,45], it is still necessary to strengthen these practices and implement policies to support migrant workers and their families in Chile in order to guarantee their psychological well-being and effective participation in society [5].
It would be beneficial to provide a support network and an effective social program involving migrants inclusively and actively in building an agenda for diagnosis and intervention on their health, labor, family, and social conditions [44,45,46]. In other countries of the Organization for Economic Cooperation and Development (OECD), state agencies or community entities have successfully implemented proposals for inclusive cities where territorial planning is open to the participation of all migrant communities to contribute to improving the quality of life and the social and economic development of the entire city [47].
As a strength, it is important to highlight that this is the first study in the country that evaluates the relationship between sociodemographic characteristics, physical and mental quality of life, and psychosocial occupational risk in migrant workers in the central-southern zone.
The study has limitations related to the medium sample size and the non-probabilistic selection. However, an attempt was made to ensure the representation of all migrant groups in the Maule region by considering the proportion by province [25] and the most frequent nationalities [29].
It is prudent to note that during 2019 and early 2020, the reality experienced by migrants in the labor market might have changed drastically due to the COVID-19 pandemic and the national economic crisis recently experienced in Chile [48]. However, more information needs to be gathered on the impact on the quality of life of the subsequent activation of employment and reopening in the country [49].
Exposure to a new social and work environment could result in different psychological responses in which anxiety, confusion, and culture shock affect the mental health of immigrants. Coming into contact with a new culture is complex, requiring support networks, adaptation, and human rights-based migration policies.
Conclusions
From the results of the study, it can be concluded that migrants with lower quality of life in the physical health dimension have lower compensation at work, low recognition from their bosses for their efforts, arrived immediately to work in the Maule region from their countries of origin and did not have a full-time job.
Migrants with lower quality of life in their mental health perceive that the amount of work exceeds the time they have available to perform their multiple tasks, have a high cognitive, sensory load, and emotional demands at work, and hide their emotions in their work. In addition, they exhibit little clarity in their work role, low support from their boss, and difficulties in social relations within the company.
Based on the above, it is recommended to implement support policies for migrant workers and their families, to guide companies on issues of labor inclusion and migration, and to strengthen the capacities of the institutions that serve the migrant population, taking into account the cultural diversity of each region, in order to ensure the welfare and effective social inclusion in Chile.