Research papers
← vista completaPublished on October 30, 2024 | http://doi.org/10.5867/medwave.2024.09.2769
Obesogenicity perception of food environments in adults: A cross-sectional study in urban areas of Santiago, Chile
Percepción de la obesogenicidad de los ambientes alimentarios en adultos: estudio transversal en zonas urbanas de Santiago, Chile
Abstract
Introduction In Chile, there is a high prevalence of obesity, and most people have an inadequate quality of food. Food environments can constitute barriers that prevent healthy food choices and lead to overweight and obesity, as well as diet-related non-communicable diseases. There are international instruments that allow the characterization of food environments. In Chile, there are no studies on the perception of food environments. This study aimed to characterize the perception of obesogenicity of food environments in the urban Chilean population using an instrument previously validated in Chile.
Methods This is a cross-sectional study with probabilistic sampling. The "Perceived Nutrition Environment Measures Survey", based on the Chilean model of food environments, was applied to 256 participants from two urban communities of the Metropolitan Region. Scores were calculated for the instrument items, which allowed calculating scores by environments included in the Chilean model of Food Environments. Negative scores were related to a higher obesogenic level.
Results The results show that the domestic food environment is perceived as less obesogenic (median of 15.8 points), with more than 90% of households having fruits, vegetables, and legumes, even though the supply food environment was negative (median -0.19 points). However, about 50% of households had ultra-processed foods. The street food environment was perceived as the most obesogenic (median -1.91 points), with more than 60% of the participants indicating difficulty finding healthy options.
Conclusions According to the level of obesogenicity of the environments studied, it is necessary to have public policies that improve them and ensure the availability and physical and economic access to healthy food, particularly in the food supply and public road environments.
Main messages
- Obesogenic food environments are common, but no studies in Chile evaluate the perceived degree of obesogenicity in food environments.
- This study shows that the domestic food environment is perceived as the least obesogenic, despite the presence of unhealthy foods in most households; the public street environment is perceived as the most obesogenic, with a low presence of healthy food sales and if they exist, they are perceived at a high cost.
- The study’s limitations are related to the selected sample of urban areas of Santiago, Chile, and in the initial period of deconfinement of the COVID-19 pandemic. In addition, the scoring system to define the perceived level of obesogenicity was not previously validated.
Introduction
Up to 40% of premature deaths from non-communicable diseases could be avoided with a healthy diet [1]. A healthy diet is defined as one that provides the nutrients necessary for good health, such as vitamins, minerals, essential amino acids, essential fatty acids, and dietary fiber and reduces potentially harmful elements such as sodium, saturated fats, and sugars [2,3]. Diets deficient in beneficial nutrients generate more deaths and years of life lost due to disability than tobacco, alcohol, and physical inactivity [4].
The last National Health Survey of Chilean adults showed that over 70% of the population has excess malnutrition [5], which has increased significantly in the last 20 years [6]. Data on schoolchildren reported figures above 50% [7]. Accordingly, the National Food Consumption Survey recorded that 95% of people require changes in their diet [8].
The characteristics of food environments may constitute barriers to choosing healthier foods such as fruits, vegetables, legumes, whole grain foods, and nuts [9,10,11]. Swinburn et al. defines food environment as the collective physical, economic, political, and sociocultural conditions influencing individuals' food and beverage choices and nutritional status, including availability, proximity, affordability, and acceptability [12]. Today, we are surrounded by obesogenic food environments. These are defined as having a high availability of unhealthy products such as ultra-processed or "high in" labeled foods, abundant commercial fast food outlets, and little access to healthy or fresh foods. For these reasons, they are recognized as risk factors for unhealthy diets and as predisposing to a high risk of chronic non-communicable diseases [13,14].
Given the evidence described, the study of food environments in Chile has become very relevant in the last decade, creating a model of these [15] based on the work of Glanz et al. [16]. The Chilean model establishes five food environments: domestic, street, institutional, catering, and supply [15]. These five environments are influenced by cultural and social dimensions, as well as by the food system and the political and socio-economic context [15].
It is essential to characterize these food environments to understand the causes of poor food and nutrition and to plan practical actions. Some standardized international instruments assess food environments. Among the most widely used is the Nutrition Environment Measures Survey (NEMS) [17]. These instruments help to identify relationships between food access and availability, demographic variables, dietary behaviors, and public policy-driven changes [14]. Only the NEMS that measures stores that sell food (NEMS-S) has been applied in Chile [18]. The NEMS-P measures the perception of the food environment. Its usefulness is based on the premise that "objectively measured food environments and perceived environments are correlated" and that perceptions influence food decisions [19]. To confirm this correlation between perceived and objectively measured environments, Alber et al. used the NEMS-P and NEMS-S, finding a significant and positive relationship between perceived and observed availability and quality of fruits and vegetables in the neighborhood (r = 0.36, p < 0.001; r = 0.34, p < 0.001) [20]. In addition, they verified that the perceived availability and quality of fruits and vegetables in the neighborhood and at home were significantly related to the daily consumption of these foods. Several investigations have concluded that, given the difficulty of directly observing food environments, perceptions measured by NEMS-P are a good approximation [20,21].
Chile has an adapted and validated version of the original NEMS-P instrument (NEMS-P-Ch) [22], which is based on Glanz et al. [16]. However, it extends the assessment to the "public road" environment of the Chilean model [15] and establishes questions on the warning labels "high in" calories, sodium, sugars, and saturated fats [23]. Despite the worldwide importance of assessing food environments, in Chile, no studies measure people’s perception of these environments, nor do they allow us to describe them or analyze their level of obesogenicity.
In this context, the present study aimed to characterize the perception of the level of obesogenicity of food environments in the urban Chilean population.
Methods
This is a cross-sectional study with probability sampling. The present study is part of a more extensive study of the Fondo Nacional de Investigación en Salud (FONIS) of the Agencia Nacional de Investigación y Desarrollo (National Agency for Research and Development). This study sought to compare the food environments of two communities in Santiago, Chile. The protocol was approved by the Ethics Committee of the Faculty of Medicine, University of Chile (Project 225-2020). Participants signed an informed consent form prior to data collection.
Adults over 18 who were responsible for household shopping participated in the study. People who could not read or write or had a disability that prevented them from understanding the questions were excluded. Also excluded were those living in the area for less than six months or planning to move within the next month because it made them less familiar with the area.
The participants lived in two communes of the city of Santiago, Metropolitan Region of Chile, one commune in the southeastern area of Santiago with low multidimensional poverty (Macul) and another in the northwestern area with high multidimensional poverty (Cerro Navia) [24]. These communes were selected by convenience, based on the possibility of working more expeditiously with the corresponding municipalities and the research team. The households to be visited were selected randomly by implementing a systematic sampling design with a random starting point, and each household was chosen at regular intervals from a georeferenced list of these obtained through each municipality [25].
The study’s sample size was calculated and estimated at 230 participants. This estimate was based on the hypothesis of no difference in the mean scores on the household food availability scale between the two municipalities. It was calculated using as a reference the study by Green & Glanz [19], which included a standard deviation of 2.5, effect size (d) = 1, probability error α= 0.05, and test power (1-β) = 0.8. We used G*Power 3.1 software for this calculation [26].
To collect information on perceptions of food environments, we used the NEMS-P-Ch questionnaire [22]. The instrument allows us to describe perceptions of the home food environment. These perceptions include the availability of healthy and unhealthy foods within the household, as well as incorporating aspects of commonality among household members; the food supply environment, including availability, access to healthy and unhealthy foods in the neighborhood, main place of food purchase, advertising in these places and appreciations of "high in" food labels; the environment, which includes the availability and access to healthy and unhealthy preparations in places such as cafeterias, restaurants and others; as well as the public food environment, which includes the availability and access to food in the streets, transport and others.
The instrument considers YES/NO responses, Likert-type scales (five options from "strongly agree" to "strongly disagree"), and frequency scales (four options from "never" to "always"). The complete instrument can be found in the project repository [27]. The questions about food environments correspond to questions that allow both to characterize the environment (e.g., "In my neighborhood, you can find...") and also to assess people-environment interactions (e.g., "I notice the black stamps when buying..."). All food availability questions were for the week prior to the survey. The instrument also includes sections to characterize the household and the person’s habits.
The research team trained the interviewers online, including the ethical information handling and the informed consent process. It also incorporated the methodology for the application of the instrument. The team collected the information by visiting the selected households between June and December 2022.
The original instrument offers a scoring system for the items but does not offer a methodology for classifying this score or determining the level of obesogenicity [19]. This is why, in this study, we proposed a new scoring methodology (raw score), ranging from -2, through -1 and 1, to 2 points for each response for the different items of each ordinal scale of the instrument. In those items with opposite meanings, this score was inverted. Thus, more negative scores are associated with being more obesogenic. Responses to descriptive questions such as "In how many places do you buy your food?" were not scored since they only described the environment or behavior of the respondent. However, no positive or negative connotation is associated with that description that would allow evaluation of the environment (e.g., shopping in two or more places does not mean that the food environment is healthier). In contrast, questions assessing the food environment, such as, "Is it easy to find fresh fruits and vegetables in the place where you buy most of your food?" were scored since they give a positive or negative connotation to the environment, according to the response. For example, the easier it is to find fruits and vegetables in a specific environment, the better the access to food, and therefore, the better the food environment.
The team decided not to work directly with the raw scores assigned by the participants to each item (Likert scale) but to proceed by recoding these scores while maintaining the same sense of the original scale, given that it was presumed that some items could have a greater degree of importance when describing the level of obesogenicity of an environment. A confirmatory factor analysis was then performed using the unweighted least squares method, obtaining factor loadings for each item. In this way, the items were grouped into different factors explaining the dimensions associated with each environment (supplementary material [27]). Those questions or items that did not present a sufficient association with any factor were excluded, according to the criterion of a factorial loading of less than 0.3, unless they were considered relevant in the research team’s opinion. Note that in order to simplify the interpretation of the factors, Varimax rotation was used. After obtaining the factorial solution, factor scores were derived. These scores represent the estimated values of the latent factors for each observation in the sample [28]. One of the most widely used methods for calculating factor scores is the regression method [29], in which the scores are derived through the product of three terms: the matrix of factor loadings, the inverse of the covariance matrix of the data, and the vector or item of interest [30]. Through this last method, it is possible to estimate the scores that are the product of a linear combination of the observed variables and finally give rise to the weighted scores.
The sum of this weighted score for each item and factor was used to calculate the scores for each environment and the total score of the instrument. The weighted scores for each factor by environment can be found in Table 1.
Medians, 25th and 75th percentile for continuous variables, and frequency and percentages for categorical variables were calculated.
Finally, the global score was divided into quintiles to facilitate its interpretation regarding obesogenicity levels. Quintiles I and II (with lower scores) had the highest potential for obesogenicity.
Results
A total of 256 people participated, of whom 67.2% were women. The median age was 54 years (between 18 and 90 years). Of those who participated, 93.8% were born in Chile, 37.9% were married, and 61.6% did not have a paid job. The median monthly household income was CLP$600 000 (approximately US$700), and households comprised between one and eight persons. The socio-demographic characteristics are shown in Table 2.
Perception of the domestic food environment
Regarding the foods that make up a healthy diet, most participants perceived that the most common fruits in the country, such as orange, banana, apple, pear, or peach (93.8%), were available in their homes. Other fruits such as blueberries, raspberries, persimmon, and pomegranate were only available in 30% of households. Vegetables such as lettuce, tomato, or celery were present in 96.1% of households. Others, such as kale, arugula, watercress, and brussels sprouts were only available in 29.7% of households. The perceived presence of legumes was present in the majority of households (91.8%). It should be noted that most of the participants perceive that healthy foods are always or almost always available in their homes (83.2%), fruits and vegetables in the refrigerator (80.9%), and these are perceived as varied (86.7%).
On the other hand, less or unhealthy foods such as cured meats (ham, salami, pate) are perceived to be present in 78.1% of households, processed meats in 64.5%, sugary drinks in 62.5%, sweets and chocolates in 57.8%, sweet or cream cookies in 52.3%, and salty snacks in 49.1%. In addition to the above, most participants perceive that they never or occasionally have availability of sweets and salty snacks (71.1%) or bakery products (82%).
The physical spaces related to home food are generally considered good or very good. For example, the place where they store food (93.7%), where they prepare food (93%), and where they consume it (94.1%). Less than 7% of the participants find the places in their homes used to store, prepare, or consume food to be harmful or average. Likewise, the time and schedule of food consumption are perceived positively (83.6% and 75% perceive them as good or very good, respectively).
Concerning mealtime variables, such as meals eaten together among household or family members, the mealtime that was always or almost always eaten together was eleven o'clock with 66.1% of the participants, followed by lunch with 48.4% and breakfast with 37.2%. About 12.5% of the sample lived alone, and about 60% did not eat dinner. The TV on during meals was always or almost always present in 57.1% of the participants at breakfast, 62.5% at lunch, and 67.5% at eleven o'clock.
The domestic food environment tends to have positive or healthy perceptions, as reflected in the fact that, in all factors, the median score is positive, with values between 0.8 and 8.3 points (Table 1). The median overall score for this environment was 15.8 points (P25 = 11.0 and P75 = 20.6) (Figure 1).
Box plots of the score obtained according to the environment studied.
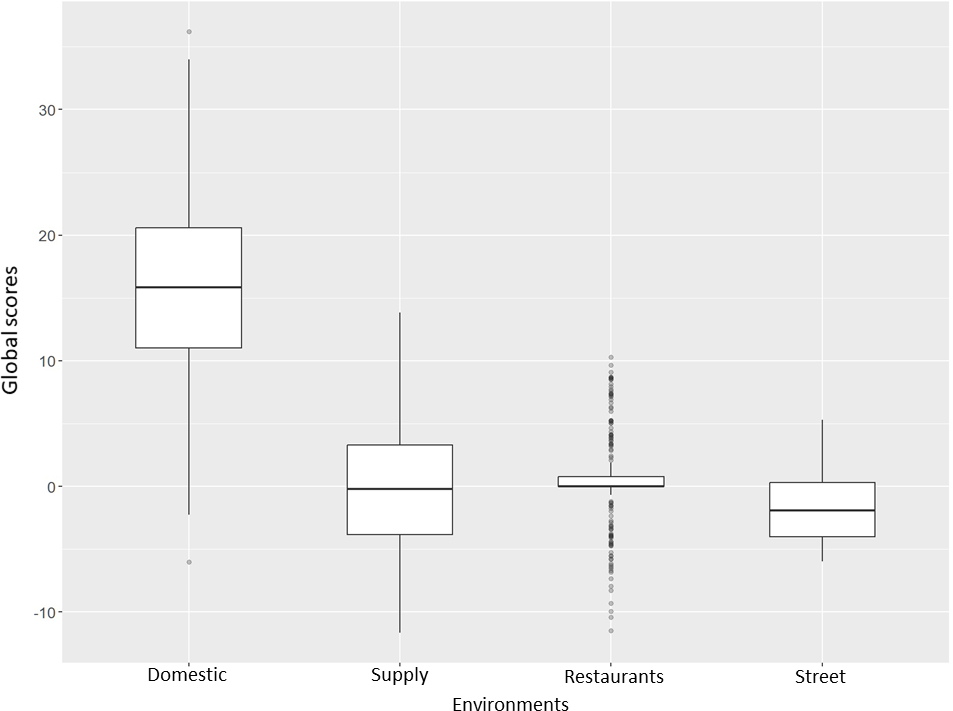
The home environment is perceived as less obesogenic. The distribution in quintiles showed a higher proportion of participants among quintiles IV (66.4%) and V (14.1%) (Table 3 ).
Perception of the food supply environment
Regarding access to healthy food, most participants perceive that they always or almost always have the facility to buy fresh fruits and vegetables in their neighborhood (90.2%) and that there is a great variety of these products (82.4%). Some 87.1% perceive that the fresh food in their neighborhood is of good quality. However, 74.2% of the participants perceive fresh fruits and vegetables as expensive or very expensive. In addition, 47.2% perceive that buying packaged foods without "high in" warning labels in their neighborhood is challenging, and 61.7% believe that there is no variety of processed foods without warning labels.
Participants indicated buying most food in supermarkets (79.3%) or fairs (77.4%). They travel to these places mainly on foot (55.1%) or by private car (38.3%). When deciding where to buy food, for the participants, it is essential to be close to home (86%), to have a variety of products (97.3%), food quality (99.6%), price (97.3%) and payment facilities (66.8%).
In these places where participants buy most of their food, they perceive that it is easy or very easy to find fresh fruits and vegetables (89.8%), fresh/canned/frozen fish (82.4%), and low-fat products (62.5%). In addition, they perceive that it is easy or very easy to buy sweets or salty snacks (96.9%) and sugary drinks (97.7%).
The highest proportion of participants indicated that they never or occasionally looked at advertising promoting the purchase of healthy foods (73%). In contrast, they perceive that there is always or almost always advertising promoting the purchase of unhealthy foods (54%) where they shop and that these foods are frequently found near checkouts (59%). However, they indicate that they never or occasionally buy foods close to checkouts (94.2%) or items at their eye level on the shelves (69.5%). Similarly, they never or occasionally read packaged foods' labeling or nutritional information (60.9%).
Slightly more than half of the participants (56.3%) indicate that "high in" warning labels on food packages influence their food purchases, while 43.8% do not.
According to the weighted scores obtained, two food supply environment factors resulted in a median negative score (more obesogenic). These factors were access to unhealthy food (-2.4 points) and availability of unhealthy food (-1.38 points) (Table 1).
Participants perceive the food supply environment as having a mostly negative, more obesogenic trend, with a median score of -0.19 points (P25 = -3.8 and P75 = 3.3) (Figure 1). Participants are distributed between quintiles II and IV of obesogenicity levels, with the majority being in quintile III (62.5%), with a median score of -0.19 points (P25 = -2.5 and P75 = 1.4) (Table 3).
Perception of the restaurant food environment
The majority of participants indicated that they did not eat meals at fast food or drive-through food outlets (69.1%), at restaurants or kitchens (61.3%), nor at carts, food trucks, or street stands (89.1%), either by delivery or by attending these outlets.
Among participants who attended or ordered food by delivery from an established food outlet (n = 124), 52% stated that choosing healthy options was always or almost always important. A total of 55.3% perceived that always or almost always the chosen location had healthy food options and that it was always or almost always easy to find preparations with fruits and vegetables (66.9%). 59.3% of 113 participants never or occasionally considered the healthy option more expensive than other food.
Regarding food promotion in these stores, most of the participants who responded (n = 122) perceived that large portions and unhealthy foods are never or occasionally promoted (53%), nor are healthy options highlighted (82.5%).
The weighted scores obtained in this environment were calculated only for those participants who answered all the evaluable items of the survey (n = 108). The median weighted scores obtained for the three factors of this environment were found to have positive values ranging from 0.99 to 1.62, with the 25th and 75th percentiles having similar negative and positive values (Table 2). In the overall environment score, participants obtained a weighted score of 1.09 (P25 = -2.9 and P75 = 5.1) (Figure 1).
The weighted scores obtained by the participants allowed their distribution among all the categories of obesogenicity level, with the majority being found among quintiles III (27.8%) and IV (26.9%), with median scores of 0.1 and 4.04 points, respectively. Almost 28% are found between quintiles I and II of the most intense level of obesogenicity (Table 3).
Perception of the street food environment
Regarding the availability of food on the street, 57.2% of participants indicated that it was important to be able to choose healthy options when they were on the street. The highest proportion of participants perceived that there were never or occasionally healthy street food outlets (72.3%), and that it was always or almost always difficult to find healthy alternatives (65.2%). Some 49.6% indicated that they could never or occasionally find fruits and vegetables for sale easily on the street. A total of 63.3% perceived that healthy options sold on the street were always or almost always more expensive. 67.2% perceived that street food advertising promotes the consumption of unhealthy foods.
The two factors in this environment obtained negative weighted scores ranging from a median of -1.33 to -1.05 points (Table 1). The median weighted score for this environment was -1.91 points (P25 = -4.0 and P75 = 0.3) (Figure 1). Participants were distributed across all quintiles of obesogenic level, with a majority between quintiles I (28.13%) and II (31.3%), i.e., more obesogenic (Table 3).
Discussion
The present study contributes to the characterization of food environments in Chile from the perception of people over 18 years of age who are in charge of food purchases through an instrument previously adapted and validated for the Chilean population, NEMS-P-Ch. The study calculated a weighted score of different factors that characterize food environments and allowed us to define the perceived level of obesogenicity. Our results showed that the domestic food environment is perceived as the least obesogenic and the street food environment as the most obesogenic.
To our knowledge, this study is the first in Chile and Latin America to propose a methodology that allows us to objectively measure the level of obesogenicity of food environments presented by the Chilean Model [15]. We can also grade it according to the quintiles created. It should also be noted that, unlike national and international evidence, the indicator created includes not only the presence of healthy foods and the absence of unhealthy ones but also incorporates dynamics and interactions that occur in these environments (e.g., family meals, reactions to warning labels, among others). Characterizing the level of obesogenic of the environments would allow us not only to propose public policies that contribute to improving them and facilitating healthy food choices in people but also to identify neighborhood, community, or regional areas that could be at a disadvantage concerning more obesogenic food environments. In this way, efforts could be focused on these groups.
In the domestic food environment, more than 90% of the people surveyed describe the presence of fruits, vegetables, and legumes, but also more than 50% describe the presence of one or more ultra-processed foods such as sausages, sugary drinks, or snacks in their homes. This is relevant considering the influence of this environment on the diet of people living at home. A previous study, which used an adapted version of the Healthy Home Survey [31], found similar results, with the presence of varied fruits and vegetables in 93.5% of households, although with a low presence of energy-dense snacks (20.5%) and sugar-sweetened beverages (6.6%) [32]. Another study in adults shows that in more than 70% of households, there is at least an apple or banana, onion, tomato, or carrot, and a low proportion of ultra-processed foods [33]. It should be emphasized that our study was conducted shortly after the end of the COVID-19 pandemic quarantine, which may have influenced the greater presence of ultra-processed foods in the home compared to previous studies, which may be related to income limitations during the pandemic and the lack of time to cook, looking for food alternatives that are quicker and easier to prepare [18,34,35].
Although the home environment has been identified as a critical element in preventing obesity [31,36], the results of our study indicate that the variables of food availability in the home and some indoor dynamics, such as eating as a family, not using screens at mealtimes, may not be sufficient to detect the real degree of obesogenicity of this environment. This is in agreement with what has been studied by Schrempft et al., who present a more comprehensive view of the home environment and its relationship with obesity, including in their study variables such as parental eating styles, the presence of playground, and the use of screens [32]. Similarly, Kegler et al. evaluated measures such as frequency of healthy meal preparation at home, portion control practices, restaurant meal consumption, and screen snacking as integrated indicators of the home eating environment [33]. On the other hand, even more complete evaluations of this environment include variables related to physical activity within the home [37], which could further complement the information regarding other dynamics and practices in the home, showing the complexity and diversity that this environment can reach.
The food supply environment, whose relationship with diet and nutrition has been widely demonstrated [38] and related to all other environments as its supplier, appears in our study as one where it is easy to find healthy and unhealthy foods. This could be a typical result in urban areas with characteristics similar to those of Santiago, Chile. However, two factors of this environment, those related to access and availability of unhealthy foods, resulted in a tendency to a more obesogenic perception, possibly due to the ease of finding this type of food. These results could indicate the existence of "food swamps", where the supply of unhealthy foods predominates, even when healthy foods are available [39]. People living in this type of environment tend to consume more unhealthy foods than others, which is why they are described as predictors of obesity [39].
On the other hand, it stands out that most of the participants perceive fruits and vegetables as high cost. It is relevant to mention that the data collection of this study was performed in a period close to the pandemic, in which food prices had increased, especially healthier foods [40], affecting the poorest people or those with fluctuating incomes, as it could have been in part of the participants of our study. Despite this, more than 90% of the participants indicated having some fruits and vegetables in their household.
It is striking in our study that people do not pay attention to the advertising or location of products in supermarkets, probably because it goes unnoticed or because this study was conducted while some communities were in confinement, so outings to buy food were less frequent. In any case, the evidence shows that the effect of advertising on food decisions is often unconscious [41,42]. In this regard, it should be emphasized that the literature shows that these strategies influence shopping choices [39].
The catering food environment could be assessed for a low percentage of participants, probably because the surveys were conducted during the initial deconfliction of the COVID-19 pandemic. More than half of the participants using this environment perceived it to be less obesogenic with availability and access to healthy menu options. This may be due to the willingness of some chain restaurants to have healthy options [43,44,45].
The street food environment was perceived as the most obesogenic, with more than 60% of people indicating that healthy foods were difficult to find and, if available, were more expensive than unhealthy ones. Thus also, most people highlight the advertising of unhealthy foods in this environment. These results are consistent with another direct observation study of street food vending around schools in Chile. It found that the presence of unhealthy foods greatly exceeded that of healthy foods [46]. Similarly, they agree with the international literature that describes the street food environment, in general, as having a high availability of unhealthy foods or preparations, nutritional imbalance, easy to consume immediately, and meager cost [47,48].
This study should be analyzed in the context of its limitations since it was conducted in only two communes in an urban area of the country’s capital, selected for convenience, adding selection biases and the impossibility of generalizing the results to a national or regional level. The scoring system that allowed us to classify the level of obesogenicity was not previously validated. However, this work follows validated procedures for other types of instruments. The study was conducted under conditions of COVID-19 pandemic deconfinement, so some perceptions of the environments studied may have been altered. Also, given the pandemic scenario that had recently occurred in the country, some selected households refused to participate in the study, probably for fear of new infections. Finally, the responses were mainly from women who did most of the household shopping and lived with another family member. This may have affected the perception of some environments.
Implications for practice
The results of this study suggest the need to continue investigating how food environments are perceived concerning their degree of obesogenic and in different contexts (for example, in rural areas, in areas that are not centralized or as urbanized as those studied in this study), or how different types of populations may perceive the same food environment (for example, Indigenous population, international migrants or other). It should be considered that this is a validated instrument that considers the five environments considered in the Chilean model and that, in addition, it is a reference for other countries in Latin America. There is also a need to generate and test interventions to improve the food environments in which the population moves daily. It is necessary to evaluate how interventions in one environment (for example, in the food supply environment) can impact other environments (for example, in the domestic environment). We hypothesize that improvements in the food supply, street, restaurant, and organizational environments would somehow improve the domestic food environment.
Also, the results of this study pose a challenge for public policies that have traditionally opted for individual rather than structural actions. An example is the insistence on nutrition education and media campaigns that promote healthy eating despite the evidence showing few favorable results [49]. We propose to work on policies that improve the availability and physical and economic access to healthy foods. In the food supply environment, this can be translated into fiscal measures (taxes and subsidies) through tax reform (of legislative order and supported by the Ministry of Finance), which would include taxes on foods defined as unhealthy (this definition is of regulatory order at the level of the Ministry of Health). In the same fiscal measures, subsidies for healthy foods have been successful. This can be established from the executive branch (Ministries of Health, Agriculture, Social Development and Education) and local authorities (regional governments and municipalities), for example, with economic support for the production of healthy foods (small producers) and the installation of free fairs and farmers' and artisanal fishermen’s markets. Other measures along the same lines are healthy food banks, which distribute baskets to the most vulnerable households. This measure can be managed by territorial governments and promoted by national funds for local projects. Another way to improve the supply and organizational environment is to implement regulatory measures (national, executive, or legislative) that prohibit the sale of unhealthy foods in protected areas such as educational and health establishments and workplaces in general. Finally, a cost-effective measure is a general ban on the advertising of unhealthy foods, a measure that, due to its scope and probable opposition, would require a legislative order [50]. Regulating the public food environment, which is currently one of the most obesogenic according to our study, requires municipal ordinances and strict guidelines for control and sanctioning in coordination with the regional (regional secretariats) and local (municipalities) levels [51].
The decision regarding the best way to influence eating behavior is complex, given the ideological difference between individual freedoms versus regulatory or legislative modification of the environments surrounding people and the more structural determinants of behavior. This is compounded by the strong opposition of some influential sectors to being regulated [52,53]. Scientific evidence and evaluation of intervention outcomes should be the key elements to consider when selecting intervention options.
Conclusions
The present study shows people’s perception of their home, food supply, street, and restaurant environments as defined in the Chilean model of food environments. The domestic food environment is perceived as less obesogenic despite having a supply environment with high levels of obesogenicity. The street food environment is perceived as obesogenic. This study reflects on the need to transform environments through public policies that ensure availability and physical and economic access to healthy food and avoid obesogenic environments. Continuing to study food environments will allow us to expand our knowledge and plan effective evidence-based interventions.
