Reporte de caso
← vista completaPublicado el 28 de abril de 2026 | http://doi.org/10.5867/medwave.2026.03.3165
Combinación poco común de adenomas oncocíticos multifocales y bocio coloide quístico calcificado en la glándula tiroides: un caso clínico
Uncommon combination of multifocal oncocytic adenomas and calcified colloid cystic goiter in the thyroid gland: A case report
Main messages
- This case report describes an exceptionally uncommon coexistence of multifocal oncocytic adenomas and a calcified cystic colloid goiter.
- The patient presented with compressive cervical symptoms, markedly elevated thyroglobulin levels, and cytology suspicious for malignancy, illustrating how benign thyroid conditions can clinically and radiologically mimic malignant disease and require comprehensive diagnostic integration.
- Imaging studies, cytology, and biochemical markers were essential to assess lesion extent and guide surgical management, highlighting the importance of a multidisciplinary approach when managing large thyroid masses, particularly in elderly patients with multiple comorbidities.
- Thyroidectomy performed in a specialized center resulted in symptom relief and satisfactory recovery, supporting evidence that carefully selected elderly patients can benefit from surgery with improved quality of life and low complication risk.
Introduction
The simultaneous presence of multifocal oncocytic adenomas and a calcified cystic colloid goiter in the thyroid gland is an exceptional circumstance that has been little documented in the medical literature [1]. Oncocytic adenomas, previously known as Hürthle cell tumors, have recently been reclassified as thyroid oncocytic adenomas by the World Health Organization in 2022, reflecting advances in understanding their origin and biological behavior [2].
Thyroid nodules are a common clinical pathology, with a prevalence of up to 65% of the adult population, which is diagnosed by ultrasound. However, only 10% of these nodules are malignant, which highlights the importance of correct diagnostic characterization to avoid both overdiagnosis and overtreatment [3].
Oncocytic adenomas are a rare entity, accounting for between 3% and 7% of differentiated thyroid tumors. Histologically, they are defined by the presence of more than 75% oncocytic cells, large, polyhedral cells with abundant, granular, eosinophilic cytoplasm resulting from the accumulation of mitochondria. Although most are benign, a small percentage may present capsular or vascular invasion, transforming into oncocytic carcinoma [4].
On the other hand, colloid cystic goiter is a benign alteration of the thyroid parenchyma caused by the growth of dilated follicles filled with colloid. Recent studies estimate that thyroid nodules affect approximately 24.8% of the world’s population, with a significantly higher prevalence in women (36.5%) than in men (23.4%). Furthermore, over the last decade, there has been a progressive increase in their detection, largely attributable to the increasingly widespread use of ultrasound as the diagnostic method of choice [5]. These lesions are often associated with degenerative changes such as hemorrhage, fibrosis, and calcification. Furthermore, thyroid calcifications are detected by ultrasound in approximately 19.8% to 32.1% of nodules, both benign and malignant [6].
The calcification pattern offers diagnostic clues: punctate microcalcifications (diameter <1 mm) are associated with papillary carcinoma in up to 79% of cases, while peripheral ‘eggshell’ calcifications are more characteristic of benign lesions such as colloid cysts [6].
Presentation of the case
This is the case of an 82-year-old female patient from the rural area of Méndez, Morona Santiago province, Ecuador. The patient has an incomplete primary education and has been working in agriculture and livestock farming. She has been living in the city of Cuenca, Azuay province, for 15 years. Her personal history includes a goiter diagnosed 30 years ago, for which she underwent a partial thyroidectomy; chronic sinusitis for 15 years; osteoporosis and high blood pressure for 10 years; type 2 diabetes mellitus for three years; hypothyroidism for eight months; and class II heart failure. She denies using tobacco, alcohol, or other substances. The patient had a two-year history of dysphagia, neck pain, and a palpable mass that progressively increased in size on the left side of her neck. The size of the mass increased significantly (Figure 1) over the course of the last month, covering the entire left side and back of the neck and the posterior region and mediastinum, causing difficulty in moving the neck, swallowing food, and breathing in, which led to the following diagnostic tests being performed.
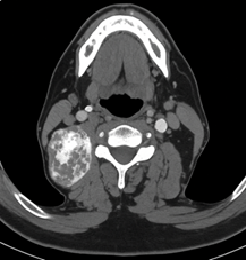
Calcified colloid cystic goiter in the thyroid gland.

At the level of the left trachea, the thyroid gland appears heterogeneous and enlarged due to the presence of a heterogeneous and irregular mass with contrast enhancement extending into the mediastinum, loss of the interface with the trachea, and inadequate interface with the esophagus. The mass measures 81 x 49 x 42 mm (Figure 2).
Computed tomography of the neck. The thyroid gland appears heterogeneous and enlarged, with an irregular mass demonstrating contrast enhancement that extends into the mediastinum.
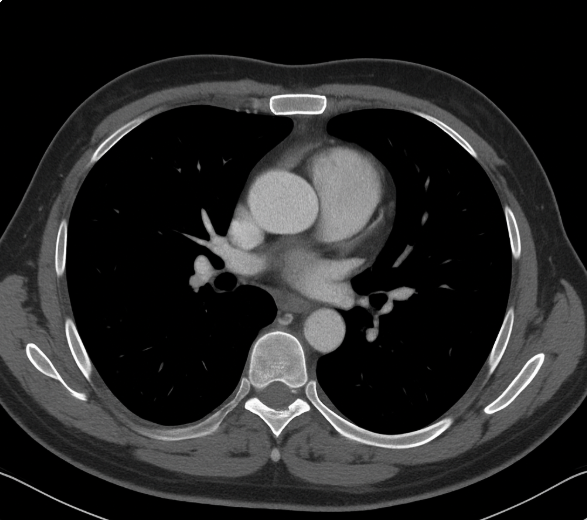
Computed tomography of the chest
No evidence of tumor activity in the lungs. Grade I cardiomegaly (Figure 3).
Computed tomography of the chest. No evidence of tumor activity in the lungs. Grade I cardiomegaly.
Blood tests Platelets 210 000, prothrombin time 11.8, prothrombin 100, International Normalized Ratio (INR) 1.00, partial thromboplastin time 25, glucose 100, urea 81, creatinine 0.92, leukocytes 7090, segmented 54.9, lymphocytes 37.5, hemoglobin 15.0, hematocrit 46.4.
Hepatitis B, C, and HIV screening: on-reactive.
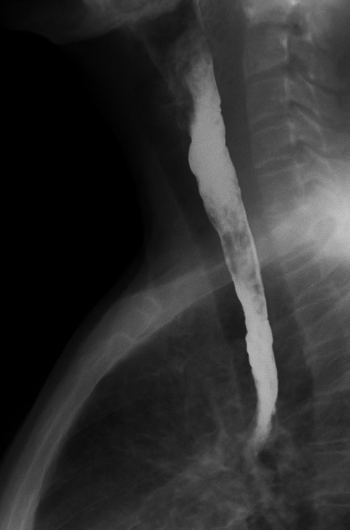
Esophagogram: Esophageal deviation to the right in its upper and middle third. No contrast leakage sites observed (Figure 4).
Esophagogram. Esophageal deviation to the right in its upper and middle third.
Left cervical mass cytology:Sydney 4: suspected malignancy (suggestive of malignancy, but insufficient characteristics or quantities).
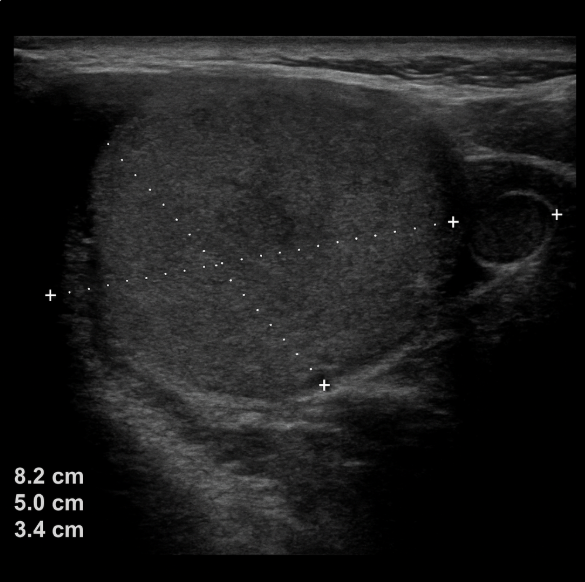
Neck ultrasound: Thyroid gland: not visible, right thyroid bed with fibro-fatty changes. A mass measuring 8.2 x 50 x 3.4 cm is observed in the left thyroid bed. Submaxillary and parotid glands: no evidence of lesions in cervical lymph nodes; some ovoid nodular images are identified, with a short axis less than 10 mm, hypoechoic and thin cortex, retaining their hilum with an echogenic center (Figure 5).
Neck ultrasound. Right thyroid bed with fibro-fatty changes.
Tumor markers: Thyroid-stimulating hormone 0.68 µUI/mL, free triiodothyronine 5.02 pg/mL, free thyroxine 1.87 ng/dL, thyroglobulin serum 11 490 ng/mL. The post-surgical data indicated a shift from a subclinical hyperthyroid state to primary hypothyroidism, as summarized in Table 1.
The patient underwent curative surgery (Figure 6), in which the left thyroid lobe, which was indurated and enlarged to 7 cm, was excised and sent for intraoperative study with a report of adenomas, goiter, and absence of the right thyroid lobe.
Thyroidectomy. Patient’s appearance during a monthly follow-up check-up.

After the operation, she was discharged six days after surgery with instructions to follow a strict liquid diet, followed by a broad liquid diet, and then a soft diet, the corresponding medication, follow-up visits every 48 hours, and a Jackson drain, which was removed four days after discharge. Short-, medium-, and long-term recovery was satisfactory, and monthly check-ups are currently being performed
Discussion
The presence of a progressively growing cervical mass in an elderly patient with a history of partial thyroidectomy poses a complex diagnostic challenge. In this case, the patient presented with compressive symptoms such as dysphagia, inspiratory dyspnea, and neck pain, accompanied by imaging findings suggestive of an expansive lesion involving adjacent structures of the neck and mediastinum. These signs, together with markedly elevated serum thyroglobulin (11 490 ng/mL) and cytology classified as Bethesda IV (suspicious for follicular neoplasia), supported the need for surgical intervention, despite the comorbidities associated with advanced age [7].
Evaluation by computed tomography scan, ultrasound, and esophagogram allowed precise delineation of the mass’s extent and its relationship to vital structures, facilitating surgical planning.
Surgery confirmed a large, indurated mass in the left thyroid bed, with no residual right thyroid tissue present. Intraoperative histopathological analysis reported a goiter with adenomas, with no conclusive evidence of carcinoma. This reinforces the findings of Kang et al. [8], who reported that thyroid nodules larger than 4 cm, even without clearly malignant cytology, can behave aggressively or exhibit compressive features warranting resection.
In older adults, thyroid surgery must be carefully evaluated, weighing the risks and benefits. In this case, the intervention was performed without major complications and with a favorable recovery, which coincides with the findings of Ng et al. [9], who demonstrated that, in experienced centers, thyroid surgery in elderly patients can be safe and significantly improve quality of life by alleviating compressive symptoms. The patient continues to undergo monthly clinical and ultrasound follow-up, with good general health and no evidence of local or systemic recurrence in the medium term.
In a cross-sectional epidemiological study conducted in China with 9,096 participants, a higher risk of thyroid nodules with a highly suspicious ultrasound pattern was identified and associated with higher weight in men and women. Therefore, it is suggested that obesity and body adiposity are associated with a higher risk of developing thyroid nodules, possibly due to mechanisms related to insulin, insulin resistance, and proinflammatory metabolic factors that stimulate thyroid cell proliferation. Adiposity measures such as body fat percentage and body mass index were found to be positively correlated with the presence of thyroid nodules, and that participants with higher body fat percentage quantiles had a significantly higher risk of having nodules of any type or with a highly suspicious ultrasound pattern (odds ratio of up to 3.10 in men) [10]. This association suggests that anthropometric characteristics related to obesity may influence the development of thyroid nodules, although the exact relationship and pathophysiological mechanisms still require further investigation. In the clinical case presented, the patient was identified as having grade II obesity with a body mass index of 38.1 kg/m², suggesting a relationship with the presence of thyroid nodules, as demonstrated by the study conducted by Itilia, which identified an association between obesity, diabetes, and nodules [11].
Finally, although the histology did not confirm malignancy, the elevation of thyroglobulin and the compressive symptoms require close follow-up, as differentiated thyroid carcinomas can present late recurrences, even decades after the initial surgery. Park et al. [12] emphasize that thyroglobulin levels are a sensitive marker of recurrence, even in the absence of suggestive radiological images. This case highlights the importance of maintaining a high index of clinical suspicion and of adequately integrating clinical, imaging, and biochemical findings in the management of patients with a history of thyroid surgery.
Conclusions
The simultaneous presence of multifocal oncocytic adenomas and a calcified cystic colloid goiter in the thyroid gland is an exceptional entity, rarely documented in the literature, which poses a diagnostic and therapeutic challenge. This case highlights the need for a comprehensive approach that combines clinical, imaging, cytological, and biochemical marker findings, given that large lesions, despite the absence of conclusive histological criteria for malignancy, may have a compressive behavior or mimic malignant neoplasms.
In older adults with significant comorbidities, the decision to operate requires a balance between risk and benefit. However, as this case demonstrates, a thyroidectomy in a specialized center can be performed safely, improving the patient’s quality of life by alleviating severe compressive symptoms such as dysphagia, dyspnea, and inability to move the neck. This is consistent with evidence that thyroid surgery in the elderly, when appropriately indicated and planned, can yield favorable outcomes and a low complication rate.
Although the histopathological study ruled out carcinoma, elevated thyroglobulin levels and surgical history require rigorous clinical, ultrasound, and biochemical monitoring, as differentiated thyroid carcinomas can recur even decades later. Continuous follow-up is essential to rule out recurrence. Furthermore, the study of such cases contributes to scientific knowledge, promoting a better understanding of the evolution and management of rare thyroid lesions.
