Review article
← vista completaPublished on April 15, 2024 | http://doi.org/10.5867/medwave.2024.03.2710
Literature review on sexuality in the elderly: What is being taught and with what technologies
Revisión de literatura sobre sexualidad en las personas mayores: qué se educa y con qué tecnologías
Abstract
Chile is facing an increasingly aging population and, with it, changes in its demographic, epidemiological, and healthcare structure. As a result, the sexual health of the elderly is an emerging area at the social level and in healthcare systems. This research aims to identify general aspects of sexuality in the elderly and learn about educational content delivered to this group using digital technologies. To do this, we proposed a review of scientific literature on the subject between January 1st, 2018, and December 31st, 2022, in the databases Web of Science, MEDLINE/PubMed, LILACS, Cochrane, Scopus, and Google Scholar. The articles found, and the emerging information was analyzed. A total of 1573 articles were found, of which 21 papers were finally included, 11 with qualitative methodology, six quantitative, and four mixed. In addition, nine addressed the area of sexuality, and 12 focused on technological innovations for the elderly. Sexuality is a growing topic worldwide, carrying with it sociocultural beliefs associated with dogmatic opinions and myths, with discrimination against this age group, especially if they belong to sexual minorities. This group also has better access to new digital technologies that facilitate access to training, social integration, and timely healthcare. Scientific evidence shows that the sexuality of the elderly is a topic of global interest, invisibilized, with low education and training of healthcare workers. The latter are neither informed nor able to solve the reasons for consultation in the traditional way or with new digital health technologies.
Main messages
- The sexuality of the elderly is an emerging and novel global phenomenon of the 21st century, highlighted by the World Health Organization, the scientific world, and, above all, by the elderly.
- The study’s limitations are that it gathers mainly qualitative literature, with databases that are not always open access, in a more limited study period, not allowing an accurate generalization of the results.
- Older people state that sexuality is important to them and that they have an active sexual life, but despite this, it is an ignored subject and the object of discrimination.
- There are gaps in the education and continuous training of healthcare personnel to educate and care for the sexuality of the elderly at primary health care, associated with a shortage of digital technologies to educate, prevent, and promote health in this stage of life.
Introduction
Population aging is a demographic phenomenon of the 21st century, and Latin America and the Caribbean are no exception. Currently, 13.4% (88.6 million) of the region’s population is made up of people aged 60 and over. It is estimated that this could increase to 16.5% by 2030, which poses challenges and opportunities in terms of public policies [1].
The World Health Organization (WHO) has proposed policies that encourage aging, the increase of healthy life expectancy, and the reduction of health inequity factors [2]. It is expected that between 2015 and 2030, the population over 60 years of age worldwide will increase from 900 million to more than 1400 million people, with an increase of 64% in just 15 years for this age group [3].
Chile is facing a similar aging population phenomenon, in addition to a decrease in mortality and fertility rates, a drop in the birth rate, an increase in life expectancy, and the gross number of the general population. However, negative vegetative growth changes are projected for those under 15 and 15 to 60 years of age towards the end of this century, so that by 2050, those over 60 are expected to outnumber those under 15 years of age for the first time [4,5].
Aging is a natural and universal process that is not uniform since social, geographical and environmental relationships determine it. Aging depends on sociocultural, family, and personal characteristics connected to the space where one is born and grows up, sexual identity, and ethnicity, among others [6]. Aging impacts sexuality throughout their life. Sexuality is understood as a central element of intimacy, companionship, and well-being, encompassing notions of sex, gender identity, roles, sexual orientation, eroticism, pleasure, intimacy, and reproduction. Furthermore, it depends on the interaction with biological, social, psychological, economic, political, social, cultural, legal, historical, and religious factors [7,8].
Sexual health, according to the Pan American Health Organization (PAHO), is understood as a state of physical, mental, and social well-being in relation to sexuality and is not the absence of disease, dysfunction, or disability [9]. This conception requires a positive and respectful approach to sexuality and sexual relations, the possibility of having pleasurable and safe sexual experiences free from coercion, discrimination, and violence. In other words, the sexual rights of all people must be respected, protected, and fully exercised [9]. Although the media and culture conceive sexual intercourse as the gold standard of sexual activity, in older people, kissing, hugging, flirting, caressing, masturbation, and bodily or emotional acts of intimacy are added [10].
In Chile, according to the fifth national survey on quality of life in old age, about 60% of older people aged 60 years and over consider that sex life is important, where 50.1% of men and 22.5% of women reported having an active sex life, especially those living with a partner (54.8%) [11]. These results coexist with social complexity and the innovations of communication and information technologies.
Access to information and communication technologies (henceforth, "technologies") among older people in Chile shows an increase of close to 40% from 2013 to date, where 50% are located between 60 and 69 years old, with high school and university education [11]. Other factors that influence the use and access to health information (age, gender, income, employment status, level of education, country or place of residence) are described. Facilitating aspects (existence of online communities, privacy, real-time interaction, or archived health information) and barriers to use (low health literacy, lack of interest, limited access, difficulty in retrieving information, unreliable health information, and distrust due to privacy concerns) are mentioned [12].
The above shows the research gap that exists in the sexuality of older people, related to the delivery of formative and informative content by healthcare workers or teams through digital media, as there is a growing need to make sexuality visible in this particular group. Accordingly, the research question is: Are technological innovations in information and communication used efficiently in older people to deliver educational content on sexuality at social, community, and healthcare centers, compared to traditional forms for the prevention and promotion of sexual health in the period considered in the research? To answer this question, this work proposes to identify general aspects of sexuality in the elderly and to know the educational content delivered to this group using digital technologies.
Methods
The present research reviews scientific literature, considering key studies in its search. The research plan included searching quantitative, qualitative, and mixed articles. The research planning included searching quantitative, qualitative, and mixed articles. Developing the selected method, we excluded papers outside the studied period or not meeting the inclusion criteria. The research question was approached through the PICO (Patients, Intervention, Comparison, Outcomes) method [13], which defined the research question.
The inclusion criteria selected for the study were persons aged 60 years and older, healthy (physically and mentally), systematic reviews and primary studies, and research conducted in Spanish, English, and Portuguese in the defined period. The exclusion criteria were participants under 60 years of age, with a severe physical disability, moderate to severe cognitive impairment, Alzheimer’s disease, protocols or unfinished research related to the subject under investigation, and studies outside the selected period.
Since this was an investigation that used secondary data, it did not consider the submission of a protocol to the ethics committee.
The search strategy contemplated a review of scientific literature from January 1st, 2018, to December 31st, 2022, by searching the Web of Science, MEDLINE/PubMed, LILACS, Cochrane, Scopus, and Google Scholar databases. The strategy aimed to find the most updated scientific publications related to the sexuality of the elderly, who were provided with educational content using innovative digital technologies in the field since digital technological innovations are scarce but recent in this age group.
The search used terms or keywords indexed according to the DeCS thesaurus for Spanish and Portuguese and MeSH for words in English, oriented to the population under study and educational interventions carried out in this group with digital technologies.
The words "older adult", "sexuality", "education", and "educational technologies'' were used. For this purpose, the Boolean operators "AND" and "OR" were used for a more specific search, such as: "sexuality and older adults", "sexuality and aging", "sexuality and older adults and technologies" "education and older adults", "older adults or education and educational technologies", "sexuality and education and aging or technologies" "sexuality and older adults", "sexuality and elderly", "sexuality and aging" "sexuality and older adults and technology", "education and older adults or elderly", "sexuality and elderly or education technology", "sexuality and aging and education or technology".
The review and search were carried out by two independent investigators, and the selection and extraction of data by two other independent investigators. This was done to avoid the risk of selection bias. These tasks were carried out under the guidance of the main investigator; the latter also settled some discrepancies that arose during both stages of the process between May and December 2022.
Likewise, research with positive and negative results was included to avoid risks of publication bias. No studies were selected from the references of the selected articles to avoid reference bias. Prior to the search, a pre-testing exercise of the planned method was performed.
The articles were saved in a database in Excel 2.0, which included forms for data collection. The first selection included the title and abstract of the articles. The pre-selected articles were analyzed in their full version for inclusion or rejection.
The final articles included were verified and entered into a form created with the following data: title, author(s), year of publication, country, scientific database, journal, objective, method, inclusion and exclusion criteria, intervention strategies, delivery of educational content, use of technologies, orientation and/or professional care, research quality, research results.
For the review and analysis of the qualitative studies, some general methodological recommendations of the ENTREQ (Enhancing transparency in reporting the synthesis of qualitative research) statement were considered. In addition, the CASP (Critical Appraisal Skills Programme) methodology was applied to validate the quality of some studies [14,15,16].
Results and evidence synthesis
Of the 21 selected articles [17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37], 43% were written in English, 38% in Spanish and 19% in Portuguese. Regarding the study method, 52% were qualitative, 29% were quantitative, and 19% were mixed. Regarding the year of publication, 19% were published in 2018, 14% in 2019, 19% in 2020, 19% in 2021 and 29% in 2022. The predominant geographic location was Europe with 43%, Latin America with 38%, and Asia with 19%.
Regarding the initial database, 37% corresponded to Web of Science, 21% to Google Scholar, 20.7% to MEDLINE/PunMed, 12.6% to Cochrane, 6.2% to LILACS, and 2.5% to Scopus.
The analysis and processing of the data found 11 qualitative, six quantitative, and four mixed studies, which were analyzed descriptively to evaluate the content of the information in accordance with the defined literature review.
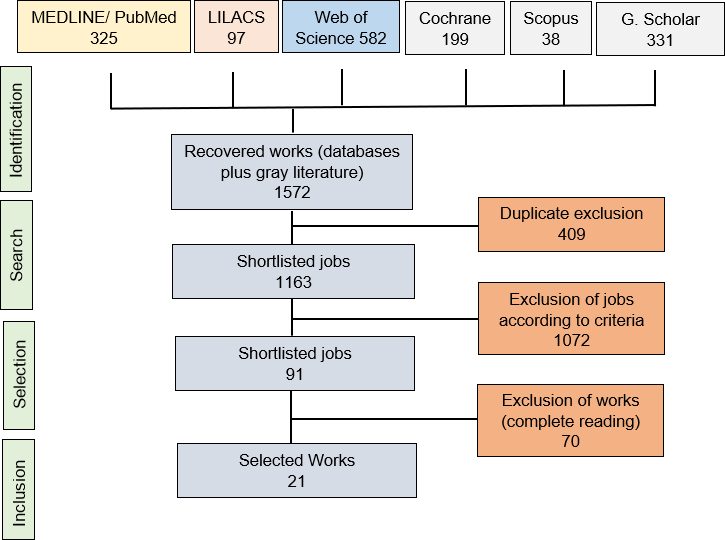
A total of 1572 research studies were obtained from all the analyzed databases. A total of 409 duplicate articles were eliminated. A total of 1163 articles were reviewed according to titles and abstracts, and 1072 articles that did not meet the research criteria were excluded. Ninety-one studies were read in full, from which 70 articles were discarded to select 21 that formed the final sample (Figure 1).
Review search scheme.
We constructed two tables summarizing the main characteristics of the included articles. Table 1 shows the articles related to sexuality in the elderly, and Table 2 shows the studies on the use of digital communication and information technologies in the same study group. In both cases, we considered whether educational content was delivered and whether healthcare workers or other related establishments developed an active role.
The quality of the reviewed studies, according to the CASP methodological recommendation [17,18,19,20,22,25,26,27,28,29,33,34,37], is high, and its main weaknesses lie in the author’s reflections on the nature of the studied subject and the depth of the ethical aspects dealt with. Seven studies were excluded for being quantitative research (Table 3).
Sexuality and elderly people
In general, sexuality is an important issue for the elderly since there is an association between an active sexual life and a better quality of life and satisfaction with one’s partner [17,18,19,20,21,22,23,24,25,38].
Lopez Ramos et al. [18] observed that sexuality is present in 60 to 79% of elderly people, more frequently in men than in women, which is in agreement with Sousa JEV et al. [21]. However, Wang V et al. [39] found the prevalence of sexual activity to be around 60%, but with no differences between sexes.
Regarding interest in sexual life, Torres and Rodriguez [19] found that more than 50% of the elderly people studied had an interest in sexual activity, expressed as optimal when there was a better state of health. However, Souza et al. mentioned that sexual interest persists despite anxiety, depression, or other mental health symptoms found [21,23,24].
Torres and Rodriguez analyzed facts that influence the sexuality of older people, such as the lack of support to enjoy sexuality in intimacy or the end of sexual life in institutionalized groups. This is consistent with the thinking of conservative Catholic older women who put an end to sexual life with widowhood, for whom the purpose of sexual relations is procreation, as a duty only for married women [19].
Physical and psychosocial conditions that influence the sexuality of elderly people
There is an association between sexuality and sexual quality of life, influenced by different biopsychosocial factors. López Ramos et al. [18] found several investigations in which they link better sexuality with better cognitive capacity, memory, and intelligence and that the quality of sexual life depends on better physical and mental capacities, which is consistent with the results of Souza et al. related to anxious and mental health disorders [21,23,24,40].
At the same time, evidence shows the relationship between quality of sexual life and comorbidities as a cause of sexual dissatisfaction. These include depression, diabetes mellitus, hypertension, osteoarticular, bladder, gastrointestinal problems, chronic pain and injuries, decreased vision, bladder pathologies, major surgeries, less energy and mobility, cognitive impairment or dementia; conditions such as decreased libido, inadequate lubrication, dyspareunia, erectile dysfunction, ejaculation difficulties, use of hormones and medications, menopause and its changes, among others [18,20].
Different research has shown that a good quality of sexual life in older adulthood depends on optimal physical and mental health, higher education and better economic income, a stable partner, preserved cognitive function, good body image perception, healthy habits, being in a stable relationship for less than five years [18,21,23,24].
Myths and beliefs about sexuality in elderly people
Several studies have mentioned the existence of myths associated with sexuality in old age [19,20,21,22,26,27]. Ricoy-Cano et al. [20] analyzed the impact on the image and sexual desire in older people as a result of maintaining active sexual relations and practicing masturbation while they were considered asexual people.
Ricoy-Cano et al. also found that women with low education and reduced economic income were educated and forced to sexually satisfy their spouses, exacerbated by the influence and stigmatization of religious ideas or gender stereotypes. Among these older people, diseases were associated with frailty [41], anxiety, marital discord, isolation, altered sexual relationships, dissatisfaction, and loss of sexual health.
Bortolozzi and Ramos [26] confirmed the social view of "asexuality" during this stage of life, which is the result of a history regulated by socio-normative codes and standards and by myths or beliefs that affect sexual health. This matches Gonzalez and Guerrero [25] regarding the stereotypes they are subjected to, and although the importance of this issue is recognized, it is invisibilized by society and blood relations.
Torres and Rodriguez [19] studied institutionalized elderly people and analyzed the causes of the loss of freedom and sexual expression and the termination of sexual life in order to avoid judgment (family and staff of the centers). In older women who followed the doctrine of the Catholic Church, the purpose of sexual relations was conception and not pleasure. The latter was associated with wifely duty rather than personal and couple enjoyment.
Elderly people, positive HIV/AIDS, and sexual minorities
In general, HIV-positive elderly people acquired the infection before this life stage and acknowledge having had little preventive education by healthcare personnel, where sexual desire is undermined by the perceived stigmatization of this disease [19].
Similarly, according to Bortolozzi and Ramos [26], the mean age of elderly people with HIV/AIDS was between 60 and 69 years. These people acquired the infection before this age, with equal frequency among men and women, with late diagnosis, psychosocial stigmatization aggravated by socioeconomic and educational risk factors, fear of lack of confidentiality, and uncertainty about their own sexuality.
Bortolozzi and Ramos analyzed the high vulnerability of elderly people to sexually transmitted infections such as HIV/AIDS, who had little information and loss of adherence to preventive practices. Healthcare professionals made sex life in old age invisible, with a lack of public policies aimed at preventive and assistance programs to minimize isolation, loneliness, fear, and shame in the face of prejudice.
De Moura Sa et al. [28] analyzed the importance of health education in older adulthood. In the case of HIV/AIDS, other authors described effective results with the validation of educational booklets for the prevention of this disease, preservation of privacy, clarification of doubts, and strengthening knowledge [42].
Healthcare personnel and sexuality education for elderly people
There is consensus in different investigations regarding healthcare personnel’s lack of preparation and delivery of educational content. Ricoy Cano et al. [20] show data regarding the low level of education in sexuality, pleasure, health, and sexual safety during aging in elderly people. Such educational deficits, according to de Souza et al., influence accelerated aging and deterioration of mental and sexual health [21,23,24].
For Bortolozzi et al., the lack of education, the discomfort of seeking healthcare, and the erroneous beliefs of health professionals increase the likelihood of risky sexual behaviors. This corroborates that elderly people think that healthcare personnel are not involved in sexual health, do not educate them nor attend to their sexual concerns or needs, and that they require preventive actions in sexual health [26].
On the other hand, Torres and Rodriguez [19] analyzed the lack of education of medical workers in sexual life during postmenopause, who need to be trained in communication skills to respond to such concerns in primary health care. Training should include social, economic, and psychological aspects, gender issues, health quality, and educational conditions, needs that Bortolozzi et al. [26] also recognized.
Similarly, Navarro [22] analyzed what was found by Moana et al. [43] about a group of nurses who, despite clinical experience, were not prepared to face a conversation on sexuality with elderly people. This topic made them uncomfortable since the training on sexual education issues referred to contraception and human reproduction in younger patients; this is consistent with Horne et al. regarding the poor training of nursing staff and care of elderly people in medical residencies [31].
Information and communication technologies for elderly people
According to Navarro [22], there is interest in using new information and communication technologies aimed at educating elderly people and encouraging innovation in teaching-learning processes. At this point, it is important not to ignore transcultural and multidimensional aspects of these people, complementing the development of competencies of those who train, together with the delivery of content in simple language to elderly people, along with the use of various technologies (computer, DVD, brochures) that strive to stimulate and motivate [27,28,30,31].
For Cardozo et al. [27], designing prototypes with an interface adapted to the needs of elderly people improved interaction with social networks through tablets. For Airola et al. [29], social networks are an important tool for learning and using technologies such as eHealth, where peers and health officials play a vital role. For their part, Lindberg and Lundgren [37] state that they are safe, flexible, and useful for scheduling hours, teaching, delivering information, and making video calls and video consultations.
However, barriers to the use of technologies have been identified that are related to the educational level of elderly people and to the ability to learn new technologies. Some frequent barriers to learning and using health technologies were cognitive and hearing difficulties, lack of connectivity, lack of simple interfaces, lack of signal or wifi, lack of prior training, lack of empowerment, and disengaged healthcare professionals [27,28,29,36,37].
Evidence also showed the importance and effectiveness of technologies in rural settings. However, it also presents limitations specific to the health of elderly people, such as obstacles to access, complexity in the use and incorporation into daily life, the design and functionality of technologies that do not always respond to the needs of people, and the lack of autonomy, among others [29,30,37].
There is a deficit in research and scientific production in matters of technology for elderly education, with a lack of investment in innovation and evaluation of technological solutions. For example, there are demonstrated gaps in access to educational technologies for these groups of interest that have sexual health demands [29].
Few interventions in elderly people promote active and healthy aging with new technologies, in addition to enabling learning, memorization, and building specific skills. In this line, there is sexual education to targeted groups to spread information and reflect on the importance of HIV prevention, with delivery of brochures used as pedagogical material on the same subject [26].
Telephone support is a useful technology that improves population coverage, reduces geographic and economic access barriers, provides proximity, and supports professional relationships with elderly people [28].
In rural settings, access to technology improves daily life and promotes social activities, physical activity, and positive aging. In addition, they allow for the informing of different programmed activities, delivering news or spreading information about the networks in which elderly people participate, and making healthcare decisions [29,30,37].
Discussion
The research shows that sexuality in elderly people is a socially invisible topic, with low participation from public health policies and a lack of preparation among healthcare workers. The study’s limitations are not having contemplated a longer period of time, applied to other databases of scientific literature, and not having found quantitative studies, which would have allowed us to analyze the heterogeneity and sensitivity of the studies, especially because there is research that is not open access. This prevents us from generalizing our findings.
Despite these limitations, the results found show an updated reality of sexuality in older adulthood, related to quality of sexual life, discrimination, relationship with healthcare personnel, access to technologies, and delivery of educational content, in line with the question and objectives answered by the research.
Several studies and authors corroborate the importance of sexuality in this study group since it is part of the quality of sexual life, understood as intimate relationships with a partner, with or without intercourse, where emotional aspects, caresses, support, masturbation, among others, also stand out [17,18,19,20,21,22,23,24,25,26,27,28,38,39].
Although the sexuality of this study group is an unveiled need, it is no less true that there are social stigmatizations against it [18,26,44]. The WHO has emphasized the global report of "ageism", understood as stereotypes, prejudices, and discrimination directed against others or self-inflicted based on age. In this case, they are directed at elderly people and exacerbated by mental health problems, progressive cognitive impairment [40], or intersectional discrimination [45].
Ageism is observed in public and private institutions, which creates and perpetuates disparities between social groups, where individual changes alone do not address ageism. This has economic and health effects on individuals [44,46].
Society and organizations are becoming more aware today of minimizing the effects of ageism or different health conditions [19,26]. However, there is discrimination against elderly people by healthcare professionals [47] or against sexual minorities such as lesbians, gays, bisexuals, and transgender people (LGBT+), so public policies of inclusion are urgently needed based on this scientific information [48,49].
The existence of myths and beliefs about the sexuality of elderly people is a reality, and these are related to sociocultural, economic, ethnographic, educational, and religious differences, among others. All this coexists with poorly trained healthcare personnel, with preventive and care gaps in this area [18,19,20,21,22,26,27].
Healthcare personnel often avoid sexual health problems and sometimes deal with them in a general way from other health consultations, with deficits in the orientation and delivery of educational content [18,19,20,21,22]. This is consistent with a lack of preparation or training [43,50] or with negative attitudes that generate significant barriers in the approach to sexuality or sexual health of elderly people [18,19,20,21,22,51].
In addition, programs should be generated to improve the sexual well-being and social impact on the health of elderly people through intermediate social determinants. For example, this can be achieved through social enterprises [52] or with smart cities that improve quality of life, sustainability, opportunities, access, mobility, and connectivity in different countries around the world [53].
Innovations in digital technologies are useful when connectivity problems are surpassed, improving social, community, and family relationships through social networks and innovations with robotic technology and artificial intelligence. These technologies are used in smartphones, tablets, personal computers, and/or smart homes [25,32,33,34,35,37,50,54] and were of great utility during the COVID-19 pandemic [36,51].
The challenges of the 21st century that relate to elderly people are gaining momentum in the midst of increasing societal complexity. In this context, universities and healthcare systems of the countries have the challenge of generating public policies in line with the increased life expectancy of elderly people. This is in order to improve the quality of life, biopsychosocial well-being, and sexual health, which must be taken into account, as it is a human right to be considered in this age group. Consequently, an important bioethical dilemma is placed as a subject for reflection.
Therefore, it is necessary to put the issue of the sexuality of elderly people on the social agenda as part of active and healthy aging policies. This should be done with an intersectional perspective [55,56] to address it from different approaches, disciplines, and integrality.
When confronting the results found with the objectives and research question, it was possible to know research with updated evidence regarding different aspects of the sexuality of elderly people. However, the educational and preventive actions confronted with digital technologies on the subject are of low effectiveness since, in general, the few studies found in the analyzed period show that they reach a low population coverage of elderly people according to the objectives set out in the research.
Conclusions
Sexuality in older adulthood is an emerging issue worldwide, which should be part of public health policies, as it is related to the well-being and quality of the sexual life of elderly people. This segment of the population deserves humanized treatment, with less ageism and more inclusiveness of sexual and ethnocultural minorities who wish to live free sexuality, with greater recognition of intimacy and sexual practices.
Technological innovations are now part of the daily lives of elderly people. Access to technologies improves the connection with the socio-environmental and ecosystemic environment and strengthens social networks where they engage in health issues; sexual health should not be an exception.
The research shows that there is limited information on educational practices on sexuality in old age on behalf of healthcare personnel. This gap increases with the low technological development of the area. This leads us to reflect on the training of healthcare personnel in this matter since the need exists and challenges us to innovate in care, education, prevention, and promotion concerning traditional forms, with a leading role in the inter and transdisciplinary.
The practice of healthcare professionals must improve at the first level of care. This is imperative based on optimal attention to the sexual health needs of elderly people from a biopsychosocial perspective and centered on the elderly person.
Research is needed to deepen this search. The delivery of knowledge on the sexuality of elderly people should be done in undergraduate health sciences careers and in postgraduate specializations, such as sexology programs, gynecology-obstetrics, gerontology, family medicine, and related scientific societies.
More evidence is needed at the national level on the level of access and resolution of the demand for sexual care for elderly people in primary health care since international evidence shows barriers at this level.
It is suggested that the scientific community deepen research on the sexuality of elderly people in the context of university medical education, at the level of health systems, with emphasis on the first level of care and in the territorial-community space.
Finally, it is necessary to join research, cooperation, and linkage efforts between institutions that produce strategies and results in the territory for a better approach to the sexuality of elderly people in education, care, and social and community inclusion.
